Gout News

Patients with gout are at increased risk of developing chronic kidney disease
Patients with gout are at increased risk of developing chronic kidney disease (CKD) than people who do not have the condition, a British study shows.
In the retrospective analysis, more than 41,000 people with incident gout (mean age 57) were matched with people without the disease. Participants were followed for a median of six years to see how many went on to develop CKD of stage 3 or worse.
While 16.2% of those with gout developed CKD stage ≥3, only 9.5% of people without gout were later diagnosed with CKD.
Those with gout had a 78 increased risk of CKD stage ≥3, the authors reported in Arthritis Research and Therapy.
Absolute rates of CKD were 28.6 and 15.8 per 10,000 person-years for those with and without gout respectively, the authors said.
Although gout has long been known to be associated with kidney disease, to the best of their knowledge, this study was the first to examine early stage CKD, the authors said.
The risk of developing CKD was highest in the first two years after gout diagnosis, when it was more than double the risk seen in people without the disease.
Adjustment for confounding factors such as age, gender, comorbidities, NSAID use, and frequency of medical visits did not change the results, the researchers reported.
An additional analysis to see whether being on urate-lowering therapy increased the risk of CKD did not show an effect in adjusted data, except in one sub-group. This group comprised women who developed CKD more than three years after gout diagnosis, and it was possible this was a chance result, they said.
The study did not prove causation, the authors cautioned.
“The association between hyperuricaemia, gout and CKD is thought to be bidirectional, with CKD known to be an independent risk factor for gout and gout potentially predisposing to CKD by a number of mechanisms,” they said.
Activation of the NLRP3 inflammasome leading to production of interleukin 1-beta was known to be a key inflammatory process in gout, they added.
“This is of note as renal NLRP3 expression is significantly increased in CKD and it has been suggested that this and interleukin 1-beta contribute to progression of CKD,” they added.
Their findings suggested that monitoring of renal function should be considered in patients with gout, they concluded.
Gout has a name-recognition problem.
Even though its prevalence is increasing dramatically in the US, many physicians don’t recognize how serious the condition can be, says N. Lawrence Edwards, MD, a rheumatologist with University of Florida Health in Gainesville and chairman of the Gout & Uric Acid Education Society. (Editor’s note: The society receives funding from pharmaceutical companies.)
“We know more about gout’s causes and genetics than any other form of the disease, yet it remains one of the most poorly treated forms of arthritis,” Edwards says.
This very painful form of inflammatory arthritis is caused when uric acid crystals accumulate in the joints. It can manifest through sudden, severe pain, redness, tenderness and swelling in the joints, and often starts with the big toe.
About 4% of American adults have gout, about double what it was 30 years ago, Edwards says. It impacts about 8.3 million Americans.
The rate is soaring because of an aging population, and is also impacted by the obesity epidemic, he notes.
Treating Short-Term Gout Attacks
To treat short-term gout attacks, doctors typically prescribe NSAIDs (non-steroidal anti-inflammatory drugs) such as Advil (ibuprofen) or Aleve (naproxen), the pain reliever Colcrys (colchicine) or corticosteroids, says Rajat Bhatt, MD, a rheumatologist in Kennewick, Washington.
Prescription NSAIDs such as Celebrex (celecoxib) can be taken at a high dose during an acute attack, and then taken at a lower daily dose to try to prevent further attacks. However, they can cause stomach pain, bleeding and ulcers.
Colchicine is used to reduce gout pain. Low daily doses might be prescribed to prevent future attacks. Side effects can include nausea, diarrhea and vomiting.
Corticosteroids, such as prednisone, can be prescribed to reduce pain and inflammation. They can increase blood sugar levels and blood pressure and may induce mood changes.
Long-Term Treatment
For many, however, gout is a chronic condition. Long-term treatment comes from medications that reduce uric acid levels. “Very good approaches have been around for a long time,” Edwards says.
This includes Zyloprim (allopurinol), a xanthine oxidase inhibitor (XOI) that reduces uric acid production. The Mayo Clinic warns that taking allopurinol during a gout attack may make the attack worse or increase the likelihood of an attack right after you’ve started taking it. Edwards says about 10% of patients can’t tolerate the drug because of stomach problems or rashes.
Uloric (febuxostat) is another XOI that can reduce uric acid production, thus reducing the frequency and severity of attacks. But it can cause joint and muscle pain and nausea.
Zurampic (lesinurad) can be prescribed along with an XOI to help reduce uric acid levels if an XOI isn’t effective enough on its own. However, the Mayo Clinic warns it can increase cardiovascular risks. It can also cause other side effects, such as headaches, flu-like symptoms and kidney stones.
If other gout medications haven’t done the trick, Krystexxa (pegloticase) can be given every two weeks as an intravenous infusion. It changes uric acid into a substance called allantoin that is easily eliminated from the body. It can cause gout flare-ups, allergic reactions and chest pain.
Deformed Toes and Relief
Larry Whited, a 78-year-old manufacturing company owner in Cleveland, was diagnosed with gout when he was in his early 50s. He was playing racquetball and initially thought he had broken his ankle. It was a gout flare-up.
He was prescribed allopurinol at the time, but “it never really broke down the uric acid in my body.” As a result of the drug not working for him, his fingers and toes became deformed and he had “pretty severe [gout] attacks on occasion.”
In 2016, Whited was referred to the Cleveland Clinic for a six-month clinical trial of Krystexxa (pegloticase). Initially he received the injection once a week for a month, and it dramatically lowered his uric acid levels. The injection frequency was lowered to once every two weeks, and he now receives it once every three weeks.
He says many others who were enrolled in the clinical trial had to drop out because of side effects, but he has not had any problems with the medication. In fact, with Krystexxa, swelling in his feet and hands decreased dramatically.
For 15 or 20 years, Derrick Mancini, a professor and distillery owner from Riverside, Illinois, would experience occasional minor gout flare-ups in his big toe, which his general practitioner told him to treat with anti-inflammatory medications. His doctor also told him to decrease his red meat consumption and to avoid beer.
Yet the flare-ups continued. “Every time, it was a little bit worse,” and gradually affected multiple toes and then his feet. Eventually “my entire foot blew up,” the 62-year-old says. His general practitioner sent him to a rheumatologist who diagnosed Mancini with chronic gout.
Mancini was prescribed Zyloprim by his rheumatologist about three years ago. He hasn’t experienced any side effects and his uric acid levels have remained relatively constant. “I have not had another bout since.”
Dietary Changes to Minimize Medicines
Although gout may be inevitable for some, dietary and lifestyle changes may reduce gout flare-ups and reduce the needs for drugs. Certain foods, such as red meat, some seafood and alcohol, are known to contain high levels of purines, substances in plant and animal food that your body converts to uric acid. Bhatt recommends a vegetarian, low-purine diet to decrease the likelihood of gout attacks. Low-purine foods include low-fat non-fat dairy products, vegetables, nuts and grains. He also recommends that patients maintain a healthy weight, as obesity is associated with gout.
The Gout & Uric Acid Education Society also recommends limiting intake of fruits that contain a high level of fructose, a naturally occuring sugar, as well as cutting back on soft drinks, which contain high-fructose corn syrup. Fruits high in fructose include apples, grapes, peaches and pears. In addition, you should avoid cereals, ice cream, candy and fast food, as they can be high in sugar and salt.
As part of the long-running Nurses’ Health Study, researchers looked at the relationship between coffee consumption and the risk of gout in nearly 90,000 women over the course of 26 years. It found a reduced risk for women who consumed coffee, according to a 2010 study published in the American Journal of Clinical Nutrition.
Meanwhile, a study published in the journal Arthritis & Rheumatism in 2012 found that consuming cherries can help reduce uric acid and was associated with a 35% lower risk of gout attacks. Eating 20 cherries a day provided the beneficial effect. Less than that number didn’t help. Using a cherry extract also helped to lower gout attacks. And combining cherries and allopurinol was found to reduce the risk of gout attacks by 75%.
Edwards says drinking cherry juice can decrease gout flare-ups, but patients who need “a uric acid medication need to stay with it for life.”
How does a diet full of processed meat affect health?By Cindi Hoover - August 4, 2018

A recent Chinese study published in the British Journal of Nutrition investigated dietary patterns and their effect on hyperuricemia, a major factor in gout.
Diet and nutrition are key factors in overall health. Previous studies suggest that certain foods are associated with various diseases related to metabolism. One example is hyperuricemia, a disease where the body has an abnormally high level of uric acid in the blood. A high level of uric acid in the blood is the main cause of gout, a type of arthritis where uric acid crystallizes in joints. High uric acid levels result from a combination of factors such as sex, age, genetics, and diet.
Researchers examined the dietary patterns of Chinese adults who were recently diagnosed with hyperuricemia. The study included 1422 adults with high uric acid levels and 1422 adults with normal uric acid levels. Their work was published in the British Journal of Nutrition.
Using a food frequency questionnaire that included 100 food items, researchers gathered information about the dietary patterns of the participants. From the information they collected, the team identified the key foods that characterize three main dietary patterns: “sweet,” “vegetable,” and “animal foods.” The main foods characterizing the “sweet” pattern were candied fruits, cookies/cakes, and ice cream. The “vegetable” pattern included high frequencies of vegetables, whole grain cereals, and soya products. Seafood, animal organs, and processed meats were the key items in the “animal foods” pattern.
Participants also answered socio-demographic questions (sex, age, and education level) and questions about lifestyle (smoking status, drinking status, sleep, and exercise frequency). They also recorded blood pressure, cholesterol, waist circumference, and other basic health measurements. Anyone who reported a major change in their lifestyle during the last five years was excluded from the study.
After adjusting for demographic and lifestyle factors, researchers found that participants with newly diagnosed hyperuricemia tended to follow the “animal foods” dietary pattern. Participants who ate lots of sugary drinks and sweet snacks were also more likely to have the disease.
By accounting for many of the behavioral, socio-demographic, and lifestyle factors, this study focuses mainly on the effect of diet on high uric acid levels in the blood. A diet full of seafood and processed meat is linked to high uric acid levels. In contrast, diets rich in vegetables are not associated with hyperuricemia.
Written by Cindi A. Hoover, Ph.D.
Reference: Xia Y et al. A dietary pattern rich in animal organ, seafood, and processed meat products is associated with newly diagnosed hyperuricaemia in Chinese adults: a propensity score-matched case-control study. 2018. British Journal of Nutrition 119:1177-1184. doi:10.1017/S0007114518000867
New American Kidney Fund Education Campaign Highlights Connection Between Kidney Disease and Gout
Email Print Friendly Share August 21, 2018 10:05 ET | Source: American Kidney Fund ROCKVILLE, Md., Aug. 21, 2018 (GLOBE NEWSWIRE) -- Aiming to demystify gout, an extremely painful form of inflammatory arthritis, the American Kidney Fund (AKF) today unveiled a new health education campaign, Goutful. The campaign debunks popular misconceptions about gout and supports kidney patients who are fighting this painful, chronic disease. A strong correlation exists between chronic kidney disease (CKD) and gout. Gout occurs when high levels of uric acid in the blood lead to crystals forming in the joints, causing inflammation and pain. One in 10 CKD patients has gout. Goutful is a play on “doubtful” and uses an educational webpage, artwork and a “Myths & Facts” quiz to debunk many of the misconceptions people have about gout—including the common beliefs that gout is the patient’s fault and that gout isn’t a serious condition. The campaign is part of AKF’s ongoing work to provide quality health education content to the CKD community and is supported by an educational grant from Horizon Pharma. “This campaign is meant to empower gout sufferers with knowledge to help them live easier and prevent further damage to their joints,” said LaVarne A. Burton, president and chief executive officer of the American Kidney Fund. “Although it can be excruciatingly painful, gout is often not taken seriously, and the patient is blamed for the condition because it is perceived to be a result of the patient’s choices. People affected by gout need resources to teach them how to manage symptoms and the painful attacks that can develop suddenly.” Gout attacks, also known as flare-ups, may occur when the body creates too much uric acid or cannot properly clear uric acid. In addition to being painful, gout flare-ups can be hard to control and often disrupt daily life such as work and family activities. Goutful dispels the following common myths associated with gout: Myth 1: “You wouldn’t have gout if you had taken better care of yourself…” Truth: Having gout is not the patient’s fault. There may be certain foods patients should avoid if they are prone to gout, and certain foods may help decrease the level of uric acid in a patient’s body, but diet alone is not a cure. People with gout who follow a healthy diet may still need medicines to prevent gout attacks by lowering the level of uric acid in their body. Myth 2: “It’s just a pain in your toe...” Truth: Gout can develop in all the joints in a person’s body and cause extremely severe pain. The big toe is the most common place for gout attacks to happen, but can happen in the hands, elbows, knees, and ankles. When people have chronic gout, often several of their joints are affected. Myth 3: “If I can’t feel it, it can’t hurt me.” Truth: Gout causes damage even when a patient is not having an attack. Symptoms of a gout attack often go away within a few days but gout is still there. Even if people don’t feel symptoms, urate crystals in the body can cause long-term health problems like joint and kidney damage. Myth 4: “I don’t need to take medicine to prevent gout if I have just a few attacks a year…” Truth: Medicine can prevent the internal damage that chronic gout causes. “With so much misinformation about gout, we’re hopeful our Goutful campaign will bring much-needed clarity to so many who struggle with this debilitating condition,” Burton said. “We are grateful for the generous support of Horizon Pharma which enabled us to develop a powerful—and empowering—campaign.” For more information about AKF’s gout campaign, visit www.KidneyFund.org/gout. About the American Kidney Fund As the nation’s leading nonprofit working on behalf of the 30 million Americans with kidney disease, the American Kidney Fund is dedicated to ensuring that every kidney patient has access to health care, and that every person at risk for kidney disease is empowered to prevent it. AKF provides a complete spectrum of programs and services: prevention outreach, top-rated health educational resources, and direct financial assistance enabling 1 in 5 U.S. dialysis patients to access lifesaving medical care, including dialysis and transplantation. AKF holds the highest ratings from the nation’s charity watchdog groups, including Charity Navigator, which includes AKF on its “top 10” list of nonprofits with the longest track records of outstanding stewardship of the donated dollar, and GuideStar, which has awarded AKF its Platinum Seal of Transparency. For more information, please visit KidneyFund.org, or connect with us on Facebook, Twitter and Instagram. Alice Andors American Kidney Fund 240-292-7053 [email protected]
Helen Fosam, PhD April 26, 2018 Examining Unmet Needs of Joint Disease Associated With Calcium Pyrophosphate Crystal Deposition
Experts recommend the development of better, unifying disease models to improve the understanding of CPPD pathogenesis and its association with OA. Credit: Biophoto Associates/Science Source
Five decades after its characterization, “pseudogout” and associated calcium pyrophosphate crystal deposition (CPPD)-related arthropathies still lack a clearly defined diagnostic and treatment strategy. One of the key challenges of treatment is that the clinical features of CPPD are often confused with those of other inflammatory joint diseases, including osteoarthritis (OA), rheumatoid arthritis (RA), and gout.1 A study of 25,157 veterans with CPPD found a positive association of CPPD with RA, hypomagnesemia, and osteoporosis.2
Positively correlated with aging, CPPD is conservatively estimated to affect approximately 3% of American adults between 60 and 69 years and as many as 50% of those older than 90 years.3,4 Between 8 and 10 million people in the United States are currently reported to be affected by CPPD,5 but the prevalence of CPPD and the associated CPPD-related arthropathies are projected to increase significantly in the coming decades in correlation with the aging US population.
Although the pathophysiology and clinical features of CPPD have been well defined,6 several aspects of the disease diagnosis and treatment are nonspecific and ill defined. For example, chondrocalcinosis on radiographic imaging of joint aspirate is often used as a surrogate indicator for CPPD, but the accuracy of this assessment is poor because of the low specificity and accuracy of the imaging. In addition, between 25% and 50% of the knee joint synovial aspirate with CPP crystals lack radiographically detectable chondrocalcinosis. There is also considerable individual and institutional variation among imaging observations, which calls into question the accuracy of CPPD diagnostic evaluation.7 Furthermore, no specific treatment is currently available to eliminate CPP crystals, and therefore the current treatment approach is primarily directed toward symptom management, including rest, ice, joint aspiration, colchicine, and intraarticular corticosteroids.6 Disease-modifying agents such as methotrexate have not shown efficacy in CPPD, and despite interest in the use of interleukin-1 inhibitor agents, their efficacy has not been demonstrated for this disease state.6 In the absence of a clearly defined management strategy, CPPD and its associated diseases will continue to present significant challenges in the future.
Addressing the challenges associated with clinical management of CPPD must start with understanding the unmet needs of associated joint damage and establishing a clearly defined strategy to address these needs. Recent progress has been made by an international group of experts from the Gout, Hyperuricemia and Crystal-Associated Disease Network (G-CAN) to advance clinical understanding of CPPD and improve its diagnosis and treatment.7 Survey questions were developed by G-CAN members, which were comprised of rheumatologists, nephrologists, and nonclinical scientists. The questions focused on key unmet needs that were broadly categorized into 6 research domains: clinical phenotyping, diagnostic modalities, pathogenesis, disease stratification, outcomes, and treatment.
A total of 140 attendees of the 2015 or 2016 G-CAN annual symposia were invited to participate in the survey. The attendees anonymously categorized the CPPD research domains according to their perceived priority. Responses were categorized as highest priority (as rated by >80% of respondents), medium priority (rated by 66.7% to 80% of respondents), and lower priority (<66.7% of respondents). A total of 26 surveys were completed; responders were residents of 10 countries across 4 continents. Highest research priorities included the need for new approaches to limit or prevent CPPD, methods to improve detection of CPP crystals in tissues and intraarticular CPPD, strategies to improve understanding of the mechanisms of disease pathogenesis, and clinical phenotyping and patient stratification.7 Based on the priorities identified, the experts provided recommendations for future basic, clinical, and translational research in CPPD.
Related Articles Ocular Complications of Gout: The Spectrum of Urate Crystal Deposition
Febuxostat vs Allopurinol Evaluated in Patients With Gout, CVDCorticosteroids May Be an Effective Alternative to NSAIDs in Acute Gout Pain
To improve the understanding of CPPD pathogenesis and its association with OA, the expert panel recommends the development of better, unifying disease models. Such models may include chondrocyte and cartilage organ culture systems, a transgenic animal model of CPPD, and gene mutational analysis to identify phenotypic heterogeneity to provide insight into idiopathic and OA-associated CPPD pathogenesis.7
“Crystal identification is paramount and does not have to be confined to joint fluid crystal analysis,” stated Robert Terkeltaub, MD, professor and chief of rheumatology at the VA Medical Center in San Diego, California, and a lead author on the study. “Specifically, urate and CPPD crystal deposits can be detected via advanced imaging by ultrasound, which appears more sensitive than plain radiography for CPPD and is certainly more sensitive than plain radiographic changes with early disease in gout. There also is a role for dual-energy [computed tomography] (DECT) in gout, although DECT has not been adequately investigated for CPPD to this point.”
Given the several different tools for assessing CPPD and to improve detection and diagnostic classification of CPPD, the panel suggests the development of internationally standardized classification criteria and consensus agreement for highly specific imaging modalities for the detection of tissue CPPD deposits. Such modalities may require improvements of high-resolution ultrasound, DECT, and magnetic resonance imaging to integrate these diverse modalities and generate a uniform CPPD diagnostic criteria.7 “Unlike the case for gout, there is not enough evidence from randomized controlled trials in acute and chronic CPPD inflammatory arthritis to craft treatment recommendations based on published, high-quality evidence” stated Dr Terkeltaub.
Consequently, to improve treatment, the panel recommends designing high-quality clinical trials of existing and emerging anti-inflammatory drugs to explore new targets and determine their safety and efficacy to treat CPP crystal arthritis. A better understanding of CPPD phenotype, and in particular, the differences between CPPD and OA and the relationship between CPPD, chondrocalcinosis, and OA can result in the improved assessment of the clinical course. The panel recognizes the need for genomic and molecular approaches in combination with well-designed prospective longitudinal studies. Implementing these research recommendations may lead to improved understanding and treatment of CPPD.
References- Macmullan P, McCarthy G. Treatment and management of pseudogout: insights for the clinician. Ther Adv Musculoskelet Dis. 2012;4(2):121-131.
- Kleiber Balderrama C, Rosenthal AK, Lans D, Singh JA, Bartels CM. Calcium pyrophosphate deposition disease and associated medical comorbidities: a national cross-sectional study of US veterans. Arthritis Care Res (Hoboken). 2017;69(9):1400-1406.
- Abhishek A. Calcium pyrophosphate deposition disease: a review of epidemiologic findings. Curr Opin Rheumatol. 2016;28(2):133-139.
- The American College of Rheumatology. Calcium Pyrophosphate Deposition (CPPD). https://www.rheumatology.org/I-Am-A/Patient-Caregiver/Diseases-Conditions/Calcium-Pyrophosphate-Deposition-CPPD. Updated March 2017. Accessed April 18, 2018.
- Rosenthal AK, Ryan LM. Calcium pyrophosphate deposition disease. N Engl J Med. 2016;374(26):2575-2584.
- Abhishek A, Doherty M. Update on calcium pyrophosphate deposition. Clin Exp Rheumatol. 2016;34(4 Suppl 98):32-38.
- Abhishek A, Neogi T, Choi H, Doherty M, Rosenthal AK, Terkeltaub R. Unmet needs and the path forward in joint disease associated with calcium pyrophosphate crystal deposition [published online April 2, 2018]. Arthritis Rheumatol. doi: 10.1002/art.40517
Do Fruits Increase Uric Acid Levels in the Blood?

Fruit is widely recommended by health organizations despite containing some sugars, including fructose. Recently, fructose has been shown to increase uric acid levels in the blood which can lead to hyperuricemia, gout, and kidney disease. A new study assessed the effect of fructose from fruit vs. sugar-sweetened beverages on blood uric acid levels.
Fructose is a common fruit sugar. It is often bonded to glucose to form the larger sugar sucrose or table sugar. Fructose is found in fruits, honey, flowers, and root vegetables. Fructose, either alone or as a part of sucrose, is commonly added to foods for taste enhancement. However, like other sugars, excessive consumption of fructose contributes to insulin resistance, obesity, and metabolic syndrome.
Recently, fructose consumption has fallen under scrutiny due to its harmful effects on the body. Fructose metabolism in the liver leads to the production of uric acid, a metabolic waste-product which is normally filtered out of the bloodstream by the kidneys. However, too much uric acid in the blood can lead to hyperuricemia, a condition that causes gout and can lead to kidney disease. This is a concerning issue due to the recent increase in added sugars to food items, including high-fructose corn syrup.
Despite this, fruit consumption is always recommended by health organizations as a low energy-dense food rich in micronutrients. This may be seen as a contradiction in nutritional advice as fructose from fruits is promoted and fructose from other foods are to be limited. Some nutritionists have questioned whether fructose from fruit has the same effects on increasing uric acid as does fructose added to other food items. To answer this question, a new study published in the American Journal of Clinical Nutrition compared the effects of fructose from whole fruit and fruit juice with a beverage with added fructose on uric acid concentration.
Does the Source of Fructose Make a Difference?
In this study, 73 patients were randomly assigned to a group to either ingest small or large servings of apples, small or large servings of apple juice, or a sugar-sweetened beverage. The researchers collected blood samples of these individuals at baseline, 30 minutes after consumption, and 60 minutes after consumption.
The researchers found that plasma uric acid concentrations increased after the intake of all fructose-containing food items, regardless of fructose source. This shows that the body responses to fructose are similar regardless of whether it is consumed from natural or artificial sources.
These results may have important implications for health nutritionists. It is possible that consuming fruits and fructose-sweetened foods throughout the day may result in a chronic increase in uric acid. However, it is not yet known whether small increases in uric acid, such as those which occur following fruit consumption, contribute to disease risk, or how long uric acid stays in the blood following fructose consumption. Long-term studies are required to assess how small and transient changes in plasma uric acid affect health.
Written by Neeti Vashi, BSc
Reference: White, S. J. (2016). The effects of apples and apple juice on acute plasma uric acid production and satiety: a randomised controlled trial (Doctoral dissertation, University of Otago).

Celery Root Can Help Treat Gout
Gout is usually associated with older people who often experience pain in the joints. But make no mistake, because gout can also affect younger people.
Usually, gout is torturous and often recurs when it is cold or raining. Now, there is a simple way that is believed to overcome gout, namely using celery root. What are the benefits?
According to herbalist dr. Erna Cipta Fahmi, if a person suffers from gout that is not too acute, self-healing can be conducted by consuming a natural herb from celery that has no side effects.
Celery is a plant that is known to have many health benefits.
Celery leaves can help treat high blood pressure. In addition, celery seeds can be used as a bronchitis ailment, and overcome problems in the liver or spleen, seizures (antispasmodic), lowering blood uric acid levels, anti rheumatism and sedation.
The root of celery, besides useful for treating gout, can also stimulate digestive enzymes and urine diuretic (diuretic).
dr. Erna also explained that celery root contains asparagine which is believed to have long been used as a food ingredient because of its delicious taste.
She also suggested when gout in the acute stage, the patient can treat gout with herbal medicine that is now widely available and easily available in herbal health clinics.
Consuming a traditional ingredient of celery root can also be used as a trusted alternative to treat gout. All you need to make this home remedy is by using celery root brewed with hot water. The celery root brew should be taken daily for 2 to 3 months.
The concoction is made from a tablespoon of celery root that has been washed and then brewed with a glass of hot water. Then closed tightly until the celery root extracts come out and the water temperature becomes normal. This celery root water can be used for two drinks in the morning and evening.
Celery root brew recipe
Ingredients
1 celery root
300 ml of water
Preparation
1. Wash the celery root, then put it in a glass
2. Pour hot water into a glass of celery root. Cover the glass, and let it cool
3. Drink ingredients celery root twice daily in the morning and evening for 2 to 3 months (For 1 cup)
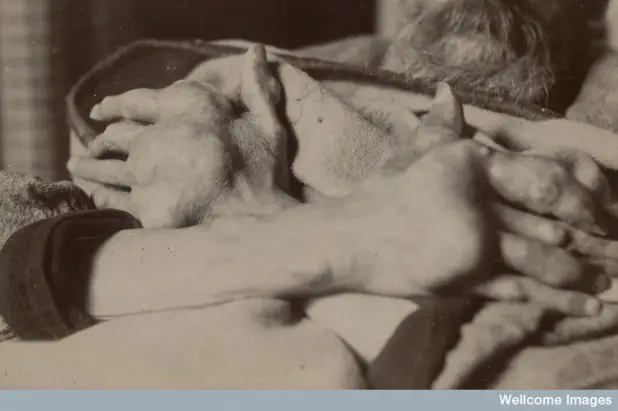
Gout and Pseudogout Updated: Mar 31, 2017 Author: Bruce M Rothschild, MD; Chief Editor: Herbert S Diamond, MD more...
Practice Essentials
Gout and pseudogout are the 2 most common crystal-induced arthropathies. Gout (see the image below) is caused by monosodium urate monohydrate crystals; pseudogout is caused by calcium pyrophosphate crystals and is more accurately termed calcium pyrophosphate disease. Gout. Acute podagra due to gout in elderly man. View Media Gallery Signs and symptoms Symptoms of gout or pseudogout include the following: Podagra (initial joint manifestation in 50% of gout cases and eventually involved in 90%; also observed in patients with pseudogout and other conditions) Arthritis in other sites – In gout, the instep, ankle, wrist, finger joints, and knee; in pseudogout, large joints (eg, the knee, wrist, elbow, or ankle) Monoarticular involvement most commonly, though polyarticular acute flares are not rare, and many different joints may be involved simultaneously or in rapid succession In gout, attacks that begin abruptly and typically reach maximum intensity within 8-12 hours; in pseudogout, attacks resembling those of acute gout or a more insidious onset that occurs over several days Without treatment, symptom patterns that change over time; attacks can become more polyarticular, involve more proximal and upper-extremity joints, occur more often, and last longer In some cases, eventual development of chronic polyarticular arthritis that can resemble rheumatoid arthritis Physical findings may include the following: Involvement of a single (most common) or multiple joints Signs of inflammation – Swelling, warmth, erythema (sometimes resembling cellulitis), and tenderness Fever (also consider infectious arthritis) Migratory polyarthritis (rare) Posterior interosseous nerve syndrome (rare) Tophi in soft tissues (helix of the ear, fingers, toes, prepatellar bursa, olecranon) Eye involvement – Tophi, crystal-containing conjunctival nodules, band keratopathy, blurred vision, anterior uveitis (rare), scleritis Complications of gout include the following: Severe degenerative arthritis Secondary infections Urate or uric acid nephropathy Increased susceptibility to infection Urate nephropathy Renal stones Nerve or spinal cord impingement Fractures in joints with tophaceous gout
Diagnosis
Studies that may be helpful include the following:
- Joint aspiration and synovial fluid analysis
- Serum uric acid measurement (though hyperuricemia is not diagnostic of gout)
- 24-hour urinary uric acid evaluation
- Blood studies (including white blood cells [WBCs, triglyceride, high-density lipoprotein, glucose, and renal and liver function tests)
Plain radiographs may show findings consistent with gout. Erosions with overhanging edges are generally considered pathognomonic for gout (though also found in other diseases). Characteristics of erosions typical of gout include the following:
- Maintenance of the joint space
- Absence of periarticular osteopenia
- Location outside the joint capsule
- Sclerotic (cookie-cutter, punched-out) borders
- Asymmetric distribution among the joints, with a strong predilection for distal joints, especially in the lower extremities
Ultrasonographic findings in established gout include the following:
- A “double-contour” sign, consisting of a hyperechoic, irregular line of MSU crystals on the surface of articular cartilage overlying an adjacent hyperechoic bony contour
- “Wet clumps of sugar,” representing tophaceous material, described as hyperechoic and hypoechoic heterogeneous material with an anechoic rim
- Bony erosions adjacent to tophaceous deposits
Other imaging modalities that may be considered include the following:
- Computed tomography (CT) – Complementary to plain radiography for recognizing erosions in gout
- Magnetic resonance imaging (MRI) – MRI with gadolinium is recommended when tendon sheath involvement must be evaluated and when osteomyelitis is in the differential diagnosis
See Workup for more detail.
ManagementGout is managed in the following 3 stages:
- Treating the acute attack
- Providing prophylaxis to prevent acute flares
- Lowering excess stores of urate to prevent flares of gouty arthritis and to prevent tissue deposition of urate crystals
Acute treatment of proven crystal-induced arthritis is directed at relief of the pain and inflammation. Agents used in this setting include the following:
- Nonsteroidal anti-inflammatory drugs (NSAIDs), such as indomethacin
- Corticosteroids
- Colchicine (now less commonly used for acute gout than it once was)
- Adrenocorticotropic hormone (ACTH)
- Combinations of drugs (colchicine plus NSAIDs, oral corticosteroids plus colchicine, intra-articular steroids plus colchicine or NSAIDs)
Therapy to control the underlying hyperuricemia generally is contraindicated until the acute attack is controlled (unless kidneys are at risk because of an unusually heavy uric acid load).
Long-term management of gout is focused on lowering uric acid levels. Agents used include the following:
- Allopurinol
- Febuxostat
- Probenecid
Because these agents change serum and tissue uric acid levels, they may precipitate acute attacks of gout. This undesired effect may be reduced by prophylaxis with the following:
- Colchicine or low-dose NSAIDs
- Low-dose prednisone (if patients cannot take colchicine or NSAIDs)
Other therapeutic agents that may be considered include the following:
- Uricase and pegloticase
- Vitamin C
- Anakinra
- Fenofibrate
Nonpharmacologic measures that may be warranted are as follows:
- Avoidance or restricted consumption of high-purine foods
- Avoidance of excess ingestion of alcoholic drinks, particularly beer
- Avoidance of sodas and other beverages or foods sweetened with high-fructose corn syrup
- Limited use of naturally sweet fruit juices, table sugar, and sweetened beverages and desserts, as well as table salt
- Maintenance of a high level of hydration with water (≥8 glasses of liquids daily)
- A low-cholesterol, low-fat diet, if such a diet is otherwise appropriate for the patient
- Weight reduction in patients who are obese
Is Rheumatology in a Rut?Cryoneurolysis Shows Promise in Treating Knee ArthritisRelieve Overloaded Physicians by Overhauling Health IT'I'm Mad as Hell!': Healthcare in America Today Hospital for Special Surgery A Simple Intervention to Improve Patient Education and Adherence in Gout Bret S. Stetka, MD; Theodore Fields, MD; Adena Batterman, MSW, LCSW
Ongoing research at the Hospital for Special Surgery (HSS) in New York City is demonstrating that an easy-to-implement, multidisciplinary approach to managing gout can significantly improve patient education and clinical outcomes. Medscape recently spoke with two of researchers behind the project—rheumatologist Theodore Fields, MD, and social worker Adena Batterman, MSW, LCSW—about how their findings can be implemented at other healthcare centers involved in gout management.
Medscape: Can you tell us how this project got started?
Dr Fields: The biggest motivation behind it was the fact that many, many gout treatment studies have shown poor outcomes. Patients just don't do well. And these studies have looked at both the community treatment of gout and treatment by rheumatologists.
If you look at how many patients get their uric acid down below 6 mg/dL—where we want them to be—around 30%-40% do not and end up doing poorly. It's been felt that often, this is an education-related issue. Patients feel better after a gout attack; they don't appreciate the importance of long-term therapy, and they stop their medicine. So, it's been widely accepted that we need better ways to get patients to adhere to their medicine.
There is also literature on self-efficacy for patients that suggests that if people understand why they're taking the medicine, it really helps. There are data looking at nurse-led treatment for gout, where the nurses would keep calling the patients and meeting with the patients. There are also data on pharmacists working with the patients and managing gout. Both approaches were successful, and we thought that because we're in a large institution, such as HSS—where we have many different disciplines under one roof—if we let each group do what they're best at and take a portion of the overall education and monitoring responsibilities, then we might be able to see better outcomes. And also, this might be something that could be replicated elsewhere.
So that was our goal: to put together a multidisciplinary team that also included social work, which Adena represents. As part of this, we wanted to make sure that anything we were giving patients was written at a reading level that everyone can understand. We want to help patients deal with financial aspects of care, and such things as transportation. We want to get them to adhere to their medicine, get the correct lab tests they need, and come back for their follow-up visits. Together, the various members of the team, we found, can help make this happen.
Medscape: You've published a clinical study testing the effects of this approach on patient outcomes, correct?
Dr Fields: Right. We decided that if we were going to do this, we really ought to study it, because maybe other groups could benefit from what we did. We decided to put together an institutional review board request and monitor what we did, and use electronic documentation that everyone involved can access.
For example, as part of the approach, pharmacists called the patients and could document the kind of issues they found, and how hard or easy it was to get the patients on the phone. Also, after patients gave consent to take part in our study, the nurse participants were able to record patient scores on a gout self-efficacy exam with 12 questions about their knowledge of gout. They were then seen by a rheumatologist, a nurse practitioner, or one of the fellows in the clinic. We then had the registered nurse meet with them to go over the answers to the survey questions and review with them with a gout education curriculum.
Every month after that, the pharmacist investigators would call the patients and inquire about whether or not they're taking their medicine, whether they know when they should be getting their lab tests done, and whether they know when their next visit with the doctor is. Then, at the 6-month mark, the nurse would meet with the patients again and administer the same test to see how their gout knowledge-based had changed or improved, and review the answers and the gout curriculum.
Because this was a pilot study, we were also very interested in what their responses were to the program itself, which was a major primary outcome for us. Did it help them to manage their gout? Did they find the program useful? What did they think of the pharmacist's input? What did they think of the nursing input? We also had the doctors, the investigators, and the noninvestigators who referred patients in to the study fill out questionnaires about what they thought of the program.The Results
Medscape: What did you find?
Dr Fields: We found that at 12 months, 85% of the patients rated the program highly for usefulness in understanding how to manage their gout, results that were published last year in Seminars in Arthritis and Rheumatism.[1] At 12 months, 81% highly rated the nursing portion of the program, and 50% of them highly rated the pharmacist program, so there was a difference between the interventions. That's something we found helpful.
Among the most frequently missed questions on the gout self-efficacy exam related to the long-term possibility of being gout-free. Patients didn't really understand that an appropriate goal was to have no gout attacks at all. Some of them still thought that having some attacks was okay. Some of them also missed the question about the important genetic component of gout. A large percentage of the patients seemed to think of gout as primarily a dietary disease.
Secondary outcomes showed that there was an improvement from a median of two gout attacks at baseline to one attack per 6 months, at 6 and 12 months. So, there was improvement. Severely painful attacks were down to 13% at 6 months and 8% at 12 months, from 60% at baseline. So, significant improvement also occurred here.
The overall takeaway from our study is that a multidisciplinary approach is a reasonable option for further study, and that other groups could benefit from some of the things that we found. Our findings could also be a guide for clinicians and researchers who are trying to develop new studies on the optimal gout management team.
Medscape: How common are multidisciplinary approaches to gout management?
Dr Fields: People have looked at similar, yet not as multidisciplinary, approaches in the past. There was research on a nurse gout management done at the University of Nottingham in the United Kingdom, and a pharmacist-led program at Kaiser Permanente in California. But no one else to our knowledge has done it with multidisciplinary groups—which we think can be effective, because the time commitment from each individual group can be lessened, and each discipline can use its special skill sets to the patient's advantage.
Medscape: Has this approach been broadly adopted yet by your institutions, HSS and Cornell?
Dr Fields: We have a large rheumatology division with about 40 rheumatologists, and the nurses for our program have all been trained to be able to give our gout questionnaire and also to be able to teach the gout curriculum to any patient who comes in. Our rheumatologists have the option of having the nurse meet with their new patients with gout, and the social workers are integral parts of the team to address psychosocial concerns. So it is in effect right now.This headline below gives really pisses me off - When do people take responsibility for their own health??
Scurvy, gout and rickets on the rise in Cornwall because of laziness and junk food binges
"Another thing about it is that no-one takes you seriously. Everyone just jokes about how you must be drinking too much port and eating too cheese. "I had a gout a few years ago now and I'm pleased to say that I haven't had it since. According to the UK Gout Society between 1997 and 2012 the prevalence of gout in the UK rose by 64%.
It has long been associated with rich food and is caused by crystals of
uric acid being deposited in the tissues when there is too much uric
acid in the bloodstream, which cannot be effectively removed from the
kidneys.
Gout often settles in the joints,
frequently in the big toe, and associated with many other serious health
conditions including obesity, kidney disease, diabetes, heart attack
and stroke. Caroline Court, Cornwall's director of public health, said there was no one reason for the re-emergence of so-called Victorian illnesses.
"There are lots of causes but some of them will be dietary factors and obesity and in some cases there is an element of deprivation involved."
The resurgence of illnesses like measles and mumps could be attributed
to the MMR jab scare a few years ago when a now thoroughly debunked
study suggested it was linked to autism.
As a result, many parents chose not to let their child
have the combined vaccine meaning the herd immunity - when a high
number of people in a community are vaccinated - was compromised.
Vaccination rates are rising again, she said, and are currently up to
about 92%, which is still below the general 95% which experts say is
necessary to prevent an outbreak. Scurvy is a rare condition that
occurs if someone doesn't have enough Vitamin C in their diet.
Sufferers become extremely fatigued, experience pain in their limbs and
small reddish-blue spots spread across the skin. It affects
mainly elderly people and those on a low income who are unable to
maintain a healthy diet but if left untreated, it can cause jaundice and
potentially fatal heart conditions.
Read more at
http://www.cornwalllive.com/scurvy-gout-and-rickets-on-the-rise-in-cornwall-because-of-laziness-and-junk-food-binges/story-30239645-detail/story.html#h3I7wgDbEHdex4fY.99
Gout vs. bursitis, differences in symptoms, causes, and treatments:
Mohan Garikiparithi
Bursitis and gout both affect the joints and can lead to inflammation and severe pain in the affected joints. Gout impacts the joint more directly than bursitis, which impacts the fluid-filled sacs that surround the joints and eliminate friction. Gout is caused by the formation of uric acid crystals, while bursitis can actually have a variety of causes, which we will go over in greater detail further on.
Another main difference between gout and bursitis is that bursitis can occur due to overuse of a certain joint, whereas this is not the case in gout. Performing repetitive motions is a key risk factor for bursitis – again, this doesn’t apply to gout.
Here, we will further explore the similarities and differences between bursitis and gout to help you better understand both of these joint conditions.
Can bursitis lead to arthritis? Bursitis and gout connection
Having gout – a type of arthritis – is a known risk factor for bursitis, but the question remains: Can bursitis lead to arthritis? The simple answer is no – although bursitis can be caused by arthritis, it does not lead to it.
Bursitis can be caused by an infection or overuse, but these can be treated, so there is no long term effect. To prevent bursitis, it’s important to avoid your triggers or modify your movements so that inflammation of the bursa doesn’t happen again.
Bursitis vs. gout: U.S. prevalenceThe worldwide prevalence of gout is one to four percent. In the U.S. specifically, 3.9 percent are affected by gout. The authors of the study Global Epidemiology of Gout: Prevalence, Incidences and Risk Factors wrote, “The prevalence of gout in more affluent countries seems to be increasing in recent decades. However, only a few studies give reliable data on secular trends in gout prevalence. The US NHANES study found a significantly higher age-adjusted prevalence (3.9 percent) in 2007–2008 than the estimate in 1988–1994 (2.9 percent). This trend paralleled an observed increase in hyperuricemia.”
Men are at a higher risk of developing gout compared to women, especially those over the age of 40. Individuals who have undergone an organ transplant are at a heightened risk for gout as well.
Bursitis accounts for 0.4 percent of primary care visits in the U.S. It is commonly seen in athletes, with incidence rates as high as 10 percent. Bursitis affects men more than women, especially those who work in construction or who are frequently kneeling.
Difference between gout and bursitis: Signs and symptoms
Typical symptoms of bursitis include pain, tenderness even without
motion, swelling, and loss of movement. If bursitis is caused by an
infection, additional symptoms – such as fever, redness of the area, and
the affected area feeling hot to touch – may be present. It’s important
to note that symptoms also depend on the location of bursitis. Here are
some additional symptoms experienced in specific locations in the body.
Hip: Pain may occur at the side of the hip and
radiate to the thigh. The hip may be painful to touch. Walking, climbing
stairs, and lying on your side becomes difficult.
Knee: Pain with movement is rare, unless the joint is significantly flexed.
Elbow: Swelling. Tenderness may occur if infection is present.
Heel: This type of bursitis is often associated with runners and is caused by overuse.
Common signs and symptoms of gout are:
Intense joint pain, especially in the large toeLingering discomfort even after the intense pain has subsidedInflammation and redness of the affected jointLimited range of motion
If a fever develops or the joint feels hot to touch, see your doctor
right away. Gout can be successfully managed as long as your doctor is
aware of your condition.
Comparing bursitis and gout causes
Bursitis is
a common cause of painful hips, knees, and elbows, but it can be
managed with nonsurgical treatments. Bursitis occurs when the bursa – a
small, fluid-filled sac that acts as a cushion and lubricator for our
bones, muscles, and tendons around our joints – becomes irritated or
infected, causing pain through movement. If bursitis is caused by an
infection, then medical treatment is required. But if no infection is
found, then medical attention can help prevent the condition from
worsening.
A person has bursitis when inflammation of the bursa occurs, causing pain when moving.
Bursitis can affect any joint, including the hip, knees, shoulder, elbow, buttocks, and thigh.
The common causes of bursitis are injury, infection, or a pre-existing condition in which crystals form in the bursa.
Gout is a result of crystallized uric acid, which occurs when a
person has high levels of uric acid in their blood. Uric acid results
from the breakdown of purines found in some foods like red meat and
alcohol.
Normally, uric acid passes through our systems and is released
through our urine, but with excessively high levels, the uric acid can
build up and crystallize in joints and surrounding tissues, causing
discomforting symptoms.
Difference between bursitis and gout: Risk factors and complications
Risk factors for gout include eating a diet high in
uric acid-promoting purines, being overweight or obese, having an
untreated medical condition like hypertension, taking certain
medications, having a family history of gout, being male over the age of
40, and recovering from a recent surgery or trauma.
Gout complications include reoccurring gout (the patient will
experience frequent flares that can cause erosion and damage to the
bones), advanced gout (nodules develop beneath the skin – these are
known as tophi and can become tender and painful during gout attacks),
and kidney stones, which can cause damage to the kidneys if they
reoccur.
Risk factors for bursitis include being of older
age, working in certain occupations such as tile laying, painting, or
playing a musical instrument. Having other medical conditions, such as
rheumatoid arthritis, gout, and diabetes, increases the risk of bursitis
as well.
Bursitis itself is an inflammation of the bursa, so when your bursa
is okay you won’t experience or develop any bursitis-related symptoms.
One main complication associated with bursitis is bunion. This is the
swelling of the first joint on the big toe, and it gets pretty painful.
If you develop bunions you should speak to your doctor about the
possibility of surgical treatment.
Diagnosis and treatment options for gout and bursitis
Unless
an infection is present, bursitis can be well managed through
self-care. It’s important to remember the acronym PRICEM when treating
bursitis at home.
Protection – Protect the area from future injuries by wearing padding.
Rest – Limit the use of the joint and let it rest.
Ice – Apply ice packs a few times a day, but not directly onto your skin.
Compression – Wear compression bandaging to limit blood flow to the area as it contributes to swelling.
Elevation – Keep the joint elevated if possible to prevent blood from pooling in the area.
Medication – Take anti-inflammatory medication or antibiotics as instructed by your doctor.
In the rare instance, surgery may be recommended to drain the bursa in order to alleviate the inflammation.
Other treatment options include physical therapy, corticosteroid injections, and assistive devices like a cane.
Some preventative means for bursitis include protecting the joints
from injury, either by wearing protective clothing or by modifying or
avoiding certain activities. Take a moment to rest if you are performing
repetitive tasks, always warm up prior to exercise, and build strong
muscles to protect your joints.
Other preventative measures include maintaining a healthy weight,
using kneeling pads, lifting objects correctly, wheeling heavy loads,
avoiding sitting for long periods of time, and exercising regularly.
Gout can also be treated with medications, including NSAIDs and other
pain relievers. Some medications can be prescribed to prevent gout
complications, including medications to block uric acid and medications
to improve uric acid removal.
Lifestyle changes and home remedies can also be implemented for
better gout management. For example, limiting alcoholic and sugary
beverages, reducing your intake of high purine foods (like red meat,
organ meat, and seafood), exercising regularly, and maintaining a
healthy weight.
Sources:
http://www.everydayhealth.com/specialists/arthritis/kitridou/qa/does-bursitis-lead-to-arthritis.aspx
http://emedicine.medscape.com/article/2145588-overview#a9
http://www.mayoclinic.org/diseases-conditions/bursitis/basics/risk-factors/con-20015102
http://www.news-medical.net/health/Bunion-Symptoms-and-Complications.aspx
Alembic gets tentative nod from US FDA for gout treatment tablet
New Delhi, July 5:
Alembic Pharmaceuticals has received tentative approval from the US health regulator for Febuxostat tablets used for treatment of hyperuricemia in patients of gout.
“The company has received tentative approval from the US Food and Drug Administration (USFDA) for its Abbreviated New Drug Application (ANDA) for Febuxostat tablets, 40 mg and 80 mg,” Alembic Pharmaceuticals said in a BSE filing.
The product is therapeutic equivalent to the reference listed drug Uloric tablets, 40 mg, 80 mg of Takeda Pharmaceuticals USA Inc, it added.
Settles case with Takeda
Alembic Pharmaceuticals said it has settled the case with Takeda and will launch its generic as per the terms of settlement.
The tablets, indicated for chronic management of hyperuricemia in patients of gout, has an estimated market size of USD 430 million for 12 months to December 2015.
The company has 48 ANDA approvals (43 final and 5 tentative) from the USFDA.
Alembic stock was trading 0.57 per cent up at Rs. 582.75 in the morning trade on the BSE.
Gouty Arthritis and Sleep Apnea: The Surprising Link You Need to Know
By Brande Plotnick
Research shows there is a link between gouty arthritis, or gout, and
sleep apnea. Gout is a painful arthritis that begins in the big toe and
is caused by a buildup of uric acid in the joints. Sleep apnea is a
condition in which breathing repeatedly pauses and restarts during your
sleep.
According to Gout and You,
a small study in the late 1980s first tied the two disorders together.
Sleep apnea lowers blood oxygen levels which in turn raises the amount
of carbon dioxide in the blood. Higher levels of carbon dioxide are
associated with higher levels of uric acid, the culprit behind painful
gout episodes.
Another study in 2012 linked snoring, often a symptom of sleep apnea,
and gout. Patients in the study who snored at least five nights each
week had higher uric acid levels.
Harvard Health Publications asserts that while there is a link between sleep apnea and gout, the exact causal relationship is not known for certain.
In addition to drops in blood oxygen levels, there is another
commonality: being overweight. Carrying excess weight increases your
risk of developing both disorders. Losing weight will not only help ward
off sleep apnea and gouty arthritis, but also countless other health
concerns.
Although the research may imply that treating sleep apnea can reduce the
risk of developing gout, scientists like Yuqing Zhang, professor of
medicine at Boston University, are not convinced. They assert that more
research is necessary to investigate whether this assumption holds true.
As for gout, the first course of treatment is often through nonsteroidal
anti-inflammatory drugs. There are also diet and lifestyle changes that
can greatly reduce the incidence and severity of the disease. For
instance, reducing intake of red meat and seafood will keep uric acid
levels in check, as will reducing your intake of alcohol and beverages
that contain high-fructose corn syrup, experts say.
Struggling with painful gout - Dr Beecraft talks symptoms, treatment and lifestyle changes

GOUT is commonly associated with older men who drink heavily - but this couldn't be further away from the truth.
Finally someone else has linked Sleep Apnea with Gout. See my article also.
A new study has found that sleep apnea is associated with an increased risk for gout, a painful disease of the big toe and other joints caused by elevated levels of uric acid in the blood.
Observational studies have shown that people with sleep apnea have a higher prevalence of excess uric acid, but until now it has been unclear whether sleep apnea is associated with gout, and how strongly.
Using records in a British health database, researchers studied 9,865 people, average age 54, with sleep apnea and matched them to 43,598 controls without the disorder. Because sleep apnea is associated with being overweight, the participants were matched for B.M.I., among many other characteristics. The study is in Arthritis & Rheumatology.
After one year, compared with controls, people with sleep apnea were about 50 percent more likely to have had an attack of gout, and the increased risk was found without regard to sex, age or obesity.
The conclusion suggests that treating sleep apnea would reduce gout attacks, but the lead author, Yuqing Zhang, a professor of medicine at Boston University, is cautious.
“Our findings call for future studies to evaluate the effect of treating sleep apnea on serum uric acid levels and the risk of gout,” he said.
FDA Advisory Committee Recommends the Approval of Lesinurad for Gout Patients
WILMINGTON, Del.--(BUSINESS WIRE)--AstraZeneca today announced that the US Food and Drug Administration’s (FDA) Arthritis Advisory Committee (AAC) voted 10-4 to recommend the approval of lesinurad 200 mg tablets for the treatment of hyperuricemia associated with gout, in combination with a xanthine oxidase inhibitor (XOI). The AAC reviewed safety and efficacy data from the pivotal Phase III combination therapy program trials, representing the largest clinical trial data set of gout patients treated with combination urate lowering therapy. The FDA is not bound by the Advisory Committee’s recommendation but takes its advice into consideration when reviewing the application for a potential medicine. The Prescription Drug User Fee Act (PDUFA) target goal date for lesinurad is December 29, 2015. If approved, lesinurad will be the first selective uric acid reabsorption inhibitor, or SURI, in the US. It inhibits the urate transporter, URAT1, which is responsible for the majority of the renal reabsorption of uric acid. Sean Bohen, Executive Vice President of Global Medicines Development and Chief Medical Officer, AstraZeneca, said: “The Committee’s positive recommendation for lesinurad is an encouraging step for patients suffering from the debilitating effects of gout, a disease in which there has been limited treatment innovation over the last 50 years. We look forward to the outcome of the FDA’s review and the opportunity to provide a new treatment option that when combined with an XOI addresses both the under-excretion and over-production of uric acid, the underlying causes of gout.” Gout is a serious and debilitating form of inflammatory arthritis caused by hyperuricemia (elevated serum uric acid (sUA)). Gout affects millions of Americans, many of whom do not reach recommended sUA treatment goals on the current standard of care (XOIs), which decrease production of uric acid. For those inadequately controlled patients, the addition of a urate lowering therapy to increase excretion of uric acid, may help them achieve treatment goals. Lesinurad is also under regulatory review in the European Union and other territories. NOTES TO EDITORS About Lesinurad If approved, lesinurad will be the first selective uric acid reabsorption inhibitor, or SURI, in the US. It inhibits the urate transporter, URAT1, which is responsible for the majority of the renal reabsorption of uric acid. By inhibiting URAT1, lesinurad increases uric acid excretion and thereby lowers serum uric acid (sUA). Lesinurad also inhibits organic anion transporter (OAT4) a uric acid transporter involved in diuretic-induced hyperuricemia. In addition, in patients, lesinurad does not inhibit OAT1 and OAT3, which are drug transporters in the kidney associated with drug-drug interactions. If approved, lesinurad in combination with an XOI would provide a dual mechanism of action to increase excretion and decrease production of uric acid enabling more patients with inadequately controlled gout to achieve target treatment goals. About Hyperuricemia and Gout Gout is a serious, chronic, progressive, and debilitating form of inflammatory arthritis. Currently, there are more than 8.3 million patients suffering from gout in the US. The underlying cause of gout is hyperuricemia (elevated serum uric acid (sUA)), which leads to the deposition of crystals primarily in the joints and in other tissues. This can result in recurrent attacks of inflammatory arthritis and, if left uncontrolled, could lead to chronic, progressive arthritis, and tophus (visible deposits of urate crystals) formation. The goal of sUA lowering treatment is to reduce sUA levels tothe target level of <6.0 mg/dL as recommended by the American College of Rheumatology (ACR). To improve signs and symptoms such as tophaceous gout, the ACR guidelines state that achieving and maintaining sUA levels <5.0 mg/dL may be required. Among patients treated in clinical trials, less than 50% of patients on allopurinol 300 mg reached serum uric acid (sUA) target levels <6.0 mg/dL. This suggests approximately two million gout patients in the US on urate lowering therapy remain inadequately controlled. For patients who cannot reach target on an XOI alone, the current ACR guidelines recommend adding an agent that increases uric acid excretion. About Ardea Biosciences Ardea Biosciences, Inc. was acquired by AstraZeneca in June 2012. It is located in San Diego, California and is a member of the AstraZeneca Group. Ardea is leading the development of AstraZeneca’s gout portfolio, including lesinurad and RDEA3170. RDEA3170 is a potent selective uric acid reabsorption inhibitor (SURI), also intended for use as a combination urate lowering therapy with xanthine oxidase inhibitors (XOIs). RDEA3170 is our lead investigational urate lowering therapy (ULT) in Asia and is currently entering a Phase IIb trial in the US. About AstraZeneca AstraZeneca (NYSE: AZN) is a global, innovation-driven biopharmaceutical business that focuses on the discovery, development and commercialization of prescription medicines, primarily for the treatment of cardiovascular, metabolic, respiratory, inflammation, autoimmune, oncology, infection and neuroscience diseases. AstraZeneca operates in over 100 countries and its innovative medicines are used by millions of patients worldwide. For more information please visit: www.astrazeneca-us.com. 3176137 10/15
Contacts
AstraZeneca
Abigail Bozarth, +1 302-885-2677
or
Melissa
Garcia, +1 301-398-6470
Gout Increases Risk of Erectile Dysfunction

Great, this is all I need to read.
Erectile dysfunction (ED) is associated with gout, whether it develops organically or psychologically, according to a new study.
For the population-based study, Chia-Hung Kao, MD, of China Medical University Hospital in Taiwan, and colleagues analyzed the medical records of 35,265 gout patients from Taiwan's national health insurance research database, 2000 to 2011. Of these, they identified patients later diagnosed with organic ED or psychogenic ED, defined as an inability to experience arousal due to mental or emotional challenges. For comparison, the investigators also examined ED incidence in 70,529 controls without gout from the general population.
After adjustment for age and comorbidities, men with gout were 1.21 times more likely to develop ED than men without a gout diagnosis, according to findings published in the European Journal of Internal Medicine. Gout patients had a 1.52 times greater risk of organic ED and a 1.18 times increased risk of psychogenic ED. ED risk was greater among gout patients with comorbidities, including chronic kidney disease, diabetes, hyperlipidemia, depression, and anxiety by 47%, 31%, 50%, 101% and 50%, respectively.
“ED is multifactorial and can be caused by vasculogenic or psychogenic problems,” the investigators stated. Among the possibilities, ED might be a gout complication, they suggested, and treating physicians should consider this risk in men with gout.
In a discussion about possible mechanisms, the researchers noted that the inflammatory response that characterizes gout can increase the risk of cardiovascular disease (via atherosclerosis and endothelial dysfunction), which has been linked with organic ED. Similarly, men with gout pain experience stress, which can contribute to psychogenic ED, possibly via cortisol. Gout treatment with glucocorticoids may also impair erection.
Among the study limitations, the investigators noted that some ED diagnoses could have made based on physicians' subjective assessment rather than the objective International Index of Erectile Dysfunction. They also could not gauge the influence of important lifestyle factors, such as obesity and smoking, or biochemical factors, such as hormone levels.
In separate study published recently online ahead of print in The Journal of Rheumatology, Wei-Sheng Chung, MD, of Taichung Hospital in Taichung City, Taiwan, and colleagues found that men with gout had a 21% increased risk of ED in adjusted analyses compared with controls without gout. Compared with patients who did not have gout or comorbidities, those with both gout and any comorbidity had a 2-fold increased risk of developing ED.
SourceFrom the 2015 Issue of Renal And Urology News »
Vultures Get Gout

Vultures are struggling to make a comeback in Indian skies. BNHS principal scientist Dr Vibhu Prakash tells Pooja Patel about vulture conservation programme of the birds in captivity
The vulture population in India had plunged by over 90 per cent, environmentalists and naturalists noted with alarm in the mid-1990s . Fifteen years on, however, the scavenging bird is back in flight with breeding centres painstakingly ensuring its revival – and survival.
Recalling how it all started, Dr Vibhu Prakash, prinicipal scientist at conservation NGO Bombay Natural History Society (BNHS), who has been studying raptors and vultures since 1984, said the Keoladeo National Park in Bharatpur, Rajasthan, had a huge vulture population till the late 1980s. But by mid-90s, their numbers dropped dramatically by almost 90 per cent. He carried out surveys in various parts of the country and found that vulture population had crashed all over. The surveys in 2007 indicated a population decline of 99.9 per cent.
"We did thorough investigation by conducting post-mortems of the dead vultures but could not pin point a real reason for the high mortality. Most vultures were found to have visceral gout, a condition when there is renal failure and the uric acid gets deposited on visceral organs. Post this, we started a vulture care centre at Pinjore, Haryana, where we brought sick vultures and worked around finding the cause of their deaths," Prakash remembers.
An American NGO, Peregrine Fund got similar findings of vulture mortality in Pakistan. But they also found residue of the non-steriodal, anti-inflammatory drug in the vulture tissues. "Post their findings, we too tested the tissues of vultures that were found dead in the country. Nearly 76 per cent vultures had died of visceral gout and all the vultures that had died of visceral gout had residue of diclofenac in their tissues. This was a clear indication that this drug was causing deaths. Diclofenac was widely used to treat cattle, and that's how the birds got it in their system too, as they feed on cattle carcasses.
In 2004, Prakash and experts from around the world discussed a recovery plan at Parwanoo in Himachal Pradesh. This plan was adopted by the Indian government in its vulture action plan. The recovery plan put forward three major recommendations — diclofenac should be banned for veterinary use, a safe alternate for this drug should be found and conservation breeding programme should be initiated. "I believed that breeding programmes, as such breeding centres, are not ideal. But if these birds were left in the wild, they would have fed on the cattle carcasses, which most likely had residues of the drug," he added.
Eight different Conservation Breeding Centres were set up across India. The objective was to release 600 pairs of each of the three species — White-backed Vulture, Long-billed Vulture and Slender-billed Vultures, in the wild. It was decided to have a founder population of 25 pairs of each of the three species in a centre. Six centres will be established in the country and release a population of 100 pairs from each centre in the wild, within 10 years of the beginning of release programme. The release programme was expected to start ten years after the founder population was collected as first year birds or nestlings.
Vultures breed only when they are six years old, that too only once a year by laying only one egg in a year. Of these, only 50% of the eggs produce successful fledglings.
"We caught juvenile birds and kept them at our breeding centres and after five to six years, they started breeding. The four centres managed by BNHS in collaboration with state governments, are in Haryana, West Bengal, Assam and Madhya Pradesh. There are four more centres that are managed by the Central Zoo Authority in Junagarh in Gujarat, Nandankanan in Orissa, Hyderabad in Telangana and Muta in Ranchi," says Prakash.
Currently, the second generation of vultures are breeding. Birds from the Haryana centre will be released in the wild next year. First two Himalayan Griffon which are not endangered will be released first and will be kept under observation and if they do not have any problems than the other species which are critically endangered will be released in the wild. The vultures will be released in flock of ten and 2-3 will be wild caught adults and rest will be captive bred 2-3 year old birds. After this, the next course of action will be sketched out.
Tomatoes Trigger Gout Pain

People who suffer from gout have long believed that eating tomatoes can
trigger a flare-up of the painful disease, and a new study from New
Zealand's University of Otago found a biological basis for their belief.
Gout is a painful form of arthritis that often attacks the big toe,
causing severe pain, redness, and tenderness. Once called the "disease
of kings" because of its link with rich food, more than 8 million
American adults have gout, and 3.9 million have been diagnosed at some
point. According to a study published in Arthritis & Rheumatism, gout affects almost three times as many men as women.
Editor's Note: Do You Have These Alzheimer's Warning Signs? Rate Your Memory Now.
Once a person has gout, particular foods can trigger a gout attack.
Otago researchers noticed that gout patients rated tomatoes as the
fourth food most likely to trigger gout, believing that only seafood,
alcohol, and red meat were worse.
"We thought it important to find a biological reason for this to add
weight to what gout patients are already saying," said researcher Tanya
Flynn.
After determining tomatoes are a commonly cited trigger food, the
authors analyzed data from 12,720 male and female patients in three U.S.
studies. The data showed that eating tomatoes was linked to higher
levels of uric acid in the blood, which is the major cause of gout.
Flynn says that while their research was not designed to prove that
tomatoes trigger gout attacks, it suggests that they can raise uric acid
levels to a degree comparable to other commonly accepted gout trigger
foods, such as seafood.
"We found that the positive association between eating tomatoes and uric
acid levels was on a par with that of consuming seafood, red meat,
alcohol or sugar-sweetened drinks," she said.
Flynn noted that the most important thing that people with gout can do
to prevent attacks is take a drug, such as Allopurinol, to reduce uric
acid levels
"Avoiding tomatoes may be helpful for people who have experienced a gout
attack after eating them, but with proper treatment this doesn’t have
to be a long-term avoidance," she said.
The study is published in the journal BMC Musculoskeletal Disorders.
Red blood cell distribution width may be useful marker of CKD in patients with gout flares
Measuring the red blood cell distribution width in patients with gout during a flare may indicate chronic kidney disease, according to researchers at the Seoul National University Hospital.
The records from 236 patients who visited the RD with acute gout attacks between March 2003 and April 2014 were retrospectively studied. The mean age of patients was 49.38 years and 92.3% were men.
Patients were divided into three groups according to tertile measurements of red blood cell distribution width (RDW). Analysis of variance (ANOVA) and Chi-square tests were used to analyze each group for any clinically relevant differences. Correlation between variables was evaluated using Pearson’s correlation approach, and multiple linear regression analysis was used to identify potentially significant influences.
Patients in the highest RDW tertile tended to be older, had lower levels of albumin and higher levels of hemoglobin, more recurrent gout flares and impaired renal function.
A “modest” negative correlation was seen with albumin and RDW and a weak, but a significant, positive correlation was revealed with creatinine levels and age. Serum uric acid and acute phase reactants were not associated with RDW. An increase in RDW independently correlated with the recurrence of gout flares and chronic kidney disease (CKD), according to the results of multiple linear regression analysis.
“In [an] acute gout attack, RDW, an easy and quick measurable index, may represent renal dysfunction rather than inflammatory burden or uric acid level, and physicians who treat acute gouty arthritis with high RDW should pay attention to the recurrence of gout attack and treatment,” the researchers concluded. – by Shirley Pulawski
Reference:
Chung SW, et al. Paper #AB0928. Presented at: European League Against Rheumatism Annual European Congress of Rheumatology. June 10-13, 2015; Rome.
Pay attention to what triggers your gout.
An acute gout attack is a throbbing, hot, painful experience, says Dr. Noel Silan, D.P.M. The condition is a form of arthritis brought on by a build up of uric-acid crystals.
Nicknamed “the disease of kings,” the condition can be triggered by a diet rich in fat and alcohol, and has become quite common in Guam due to the local diet, Silan adds.
“My first episode actually wasn’t as bad as my second, only because my pain tolerance was high when I was 25,” says John Calvo, who suffers from gout. “I just thought I had a broken toe. I’m a grappler and was a professional fighter back then, so I got injuries all the time. The doctor did X-rays and nothing was wrong. Blood work was done. Doc said it showed uric acid levels of a 40 year old.”
“The second attack at 37, though … I woke up in pain. Someone just walking by me hurt,” Calvo adds.
An acute gout attack usually happens overnight and typically affects the big toe, feet, ankles, knees, and hands. During sleep, the body’s core temperature drops. The toe is the furthest extremity from the body, so it’s the coldest overall. In Guam, most people also sleep with a fan or air conditioner running. The toe’s temperature drops even more, explains Silan.
Toes also have the lowest circulation of blood, making it the perfect nesting place for uric acid to crystallize and cause pain, says Silan. He’s even advised his patients to try wearing warm socks to bed, which he says has resulted in positive feedback.
Dr. Noel Silan, D.P.M. uses three anti-inflammatory injections to combat an acute gout attack.
What not to eat
Uric acid, the culprit of gout pain, is a byproduct of purine metabolism. It’s also considered an anti-oxidant, says Dr. Silan.
They are found naturally in every living organism, animal and plant. For those suffering from gout, there is a long list of high-purine foods to avoid, but the best way to approach it is to just pay attention to the trigger foods, says Dr. Silan.
High-protein meats have more purine than plants. Beans have more purine than greens. Organ meat has more purine than muscle meat. Beer has more than other alcohols because of the yeast.
For Calvo, a gout attack often occurs after a few beers.
“If I drink beer; especially craft beers, those are my triggers. Light beer has no effect. Pork has no effect. My brother, his trigger was shellfish. My dad, it was pork.”
Obesity
Obesity is also a high-risk factor for gout. Calvo noticed the frequency of gout attacks increased as he gained weight and became less active.
Weight loss at a slow rate is recommended. Losing weight quickly, raises uric acid levels quickly. Since purine is in every cell, a breakdown of cells can raise uric acid levels. Cancer patients going through treatment have cells breaking down quickly and are more prone to gout, says Silan.
Remedies
Dr.
Noel Silan, D.P.M. points to an X-ran of a toe joint that shows erosion
due to long term gout. He recommends immediate treatment and
maintenance.
To help alleviate a gout flare up immediately, apply ice to the swelling and then take an anti-inflammatory medicine.
“I have patients who try to control it on their own, but they’re going to limp around for days or weeks,” says Dr. Silan.
It’s better to seek treatment immediately. Silan says his treatment makes the pain dissipate in a few hours because it attacks the inflammatory process in three different pathways.
“I’ve been practicing since 1997 and almost everyday or every other day, I have a patient with gout come in,” says Silan. “It is very common in Guam because of the diet. Usually the patient had a weekend of celebrating with food-laden fiestas and barbeques.”
It’s very important to control gout. Long-term increased uric acid levels begin distributing into the larger joints, attacking knees and elbow joints.
Long-term maintenance involves diet, exercise and keeping hydrated.
If it’s still not under control, then allopurinol, a medication that stops the production of uric acid; or colchicine, a stronger than over-the-counter anti-inflammatory medication; or a combination of both is added to the regiment.
Salt dehydrates the body. Without dilution, uric acid becomes concentrated and crystallizes. Canned meat has not only a high sodium chloride, i.e. salt content but also sodium nitrate. Stay away from fast running fish like sardines, anchovies, dilis or maña hak. They have high salt content as well.
Caffeine not only dehydrates the body, but it competes with uric acid in the kidneys, which can also lead to gout flare up.
Medscape Medical News Gout Limits Function of Lower Extremities in Older Adults
Older adults with gout and hyperuricemia are more likely to have worse lower extremity function than their peers, but their upper body function appears to be similar, a study has shown.
Lower extremity function is especially poor in patients with gout who are older, who have a higher body mass index, who are of black race, and who have a history of stroke, diabetes, and osteoarthritis, Bridget Teevan Burke, MS, MPH, from the Department of Epidemiology, Johns Hopkins University Bloomberg School of Public Health, Baltimore, Maryland, and colleagues report in an article published online July 2 in Arthritis Care & Research.
To assess the relationship between physical function and gout and hyperuricemia, the investigators conducted a cross-sectional analysis comprising 5819 individuals from the ongoing, prospective Atherosclerosis Risk in Communities (ARIC) study who had self-reported gout status, hyperuricemia data, and available physical function measurements. The physical function measures include the Short Physical Performance Battery (SPPB), grip strength assessment, and a 4-m walking test.
Of the 5819 participants, 10% reported a history of gout, and 21% had hyperuricemia. The physical function analysis showed that participants with gout performed worse than those without gout on the SPPB. The prevalence odds of a 1-unit increase in their SPPB score were 0.77, and they were 1.18 times more likely to have a poor SPPB score, the authors report.
Although the association between gout and SPPB score was not different between men and women, the association between gout and poor SPPB performance was greater in men, the authors observe.
With respect to walking speed, patients with gout had slower walking speeds and were 1.19 times more likely to have poor walking speed than those without gout, and the association between gout and poor walking speed was greater in men, the authors report.
There was no difference in grip strength by history of gout overall and by sex, according to the analysis.
As with gout, patients with hyperuricemia had worse SPPB scores and walking speeds, but no difference was observed by grip strength, the authors write.
The investigators analyzed the data for predictors of poor physical function. Among older adults with gout, the likelihood of poor SPPB score increased with every 5-year increase in age (prevalence ratio [PR], 1.27; 95% confidence interval [CI], 1.16 - 1.39), as well as for every 5 kg/m2 increase in BMI (PR, 1.10; 95% CI, 1.02 - 1.19). Poor SPPB score was also more alike for subjects who were black (PR, 1.35; 95% CI, 1.09 - 1.66), current smokers (PR, 1.45; 95% CI, 1.04 - 2.04), and those with a history of stroke (PR, 1.47; 95% CI, 1.06 - 2.04), diabetes (PR, 1.54; 95% CI, 1.27 - 1.88), and osteoarthritis (PR, 1.60; 95% CI, 1.25 - 2.03), the authors report, noting that similar factors for poor walking speed were identified.
Sensitivity analyses showed that the association between hyperuricemia and physical function was similar among participants with and without a history of using gout medication, and that disease duration was not associated with physical function performance.
Although the researchers expected that older adults with gout and hyperuricemia were likely to have worse physical function overall, "We were surprised to see that these associations were limited to lower extremity function," according to principal investigator Mara McAdams DeMarco, PhD, assistant professor, Department of Epidemiology, Department of Surgery, Johns Hopkins. "However, this makes sense, given that the most common localizations of affected joints are in the lower extremity. Patients with gout are most likely to be first affected by lower extremity joints."
Although previous research has focused on irreversible joint damage resulting from gout, "our study suggests that prior to the onset of joint damage, those with gout are at risk of poor physical function," Dr DeMarco told Medscape Medical News. "This deficit in lower extremity physical function is associated with increased risk of mortality in older adults."
The findings also have relevance to clinical practice, Dr DeMarco noted. "Physicians can recognize these high-risk subgroups of older adults with gout in their clinical population and potentially counsel the patients on the benefits of exercise to improve lower extremity physical function."
This study was jointly funded by the Arthritis National Research Foundation and the American Federation for Aging Research. The authors have disclosed no relevant financial relationships.
Arthritis Care Res. Published online July 2, 2015. Abstract
Pharmacy finger prick tests for gout patients investigated
Reynald Castaneda[email protected]
Related Stories GP vs pharmacist: Lack of funds for warfarin devalues doctors Warfarin service under review before expansion
Patients suffering from gout could soon be able to get their uric acid levels tested at pharmacy.
A
Counties Manukau DHB community pharmacy services agreement document
says the service sees pharmacists being able to measure a patient’s uric
acid levels via a finger prick test using a point of care device.
In collaboration with a GP, the pharmacist would then be able to adjust the patient’s dose of allopurinol.
Pharmacy would also be given responsibility in educating patients on how to manage gout, the document says.
It says a pilot has been proposed in conjunction with health innovation centre Ko Awatea.
Pharmacy’s warfarin management service, which this gout service is being compared to, had drawn criticism from GPs in the past.
The
document was released as an appendix to Counties Manukau DHB’s
community and public health advisory committee (CPHAC) minutes for a
meeting held this month.
Counties Manukau DHB and Ko Awatea representatives could not be reached in time for deadline.

Seafood Protein Ups Gout Risk in Chinese Patients
Singaporean study also notes dietary intakes of soy and legumes may reduce risk.
-
by Wayne Kuznar
Contributing Writer
Action Points Poultry, fish, and shellfish as the main sources of dietary protein led to an increased risk of gout while plant-based proteins reduced the risk.Note that consumption of soy food and legumes was associated with a reduced risk of gout.
Poultry, fish, and shellfish as the main sources of dietary protein led to an increased risk of gout, according to a study from Singapore, while plant-based proteins reduced the risk.
Based on long-term data from a population-based study, Chinese participants who developed gout had greater consumption of total protein, red meat (including pork, beef, and lamb), poultry, fish, and shellfish at baseline compared with those not diagnosed with gout, reported Gim Gee Teng, MBBS, MD, of the National University Health System, and colleagues.
Advertisement
In a multivariate-adjusted model (all P-values for trend), the risk of incident gout was significantly higher among subjects in the highest quartile of poultry consumption relative to the lowest (hazard ratio 1.27, 95% CI 1.11-1.45, P<0.001) and among those in the highest quartile of fish and shellfish consumption (HR 1.16, 95% CI 1.02-1.32, P=0.006) relative to the lowest quartile, the authors wrote in Arthritis and Rheumatology.
Additionally, those with total protein intake in the highest quartile had a significantly increased risk of gout compared with those with intake in the lowest quartile (HR 1.27, 95% CI 1.12-1.44, P<0.001). In contrast, soy protein consumption in the highest quartile was associated with a reduced risk of gout compared with consumption in the lowest quartile (HR 0.89, 95% CI 0.79-1.01; P=0.06).
Patients with gout are generally advised to avoid all sources of protein even though data about which sources of protein are most harmful are unclear, the authors noted.
"The present study demonstrated that among the Chinese population in Singapore, higher consumption of poultry, fish, and shellfish, but not eggs, nuts, seeds, and grain products, was associated with an increased risk of gout. This is also the first prospective study to show a possible protective association of soy foods and legumes on the risk of developing gout."
The investigators analyzed data from the Singapore Chinese Health Study. They examined the relationship between dietary intake of protein and its sources and incident gout in 63,257 Chinese adults, ages 45 to 74 at baseline.
A food frequency questionnaire captured the participants' dietary habits in the preceding year. Two follow-up interviews were conducted to determine participants' medical histories, including whether they had been told they had gout, and to update information on lifestyle factors.
A total of 54,431 participated in either or both of the follow-up interviews. After exclusions for baseline cancer, extreme caloric intake, prevalent gout before baseline, and missing age of gout diagnosis, the analysis included data from 51,114 subjects.
After a mean follow-up of 11.1 years, there were 1,151 new cases of gout diagnosed by the first follow-up and 1,016 by the second follow-up, for a total of 2,167 cases.
The mean age at diagnosis was 61.3. The authors noted that the incidence rates of gout standardized to the age structure of the whole cohort were 504 per 100,000 person-years in men and 294 per 100,000 person-years in women.
"The consumption of red meat was positively associated with risk of gout, but this was attenuated after additional adjustment for other dietary variables," they wrote.
Consumption of soy food and legumes, in contrast, was associated with a reduced risk of gout. Those among the highest consumers of soy had an HR of 0.86 (95% CI 0.75-0.98, P=0.018) for incident gout relative to the lowest quartile of consumers of soy, and those in the highest quartile of legume consumption had an HR of 0.83 (95% CI 0.73-0.95, P=0.012) compared with those with consumption of legumes in the lowest quartile.
When analyzed by gender, the positive association between gout and fish and shellfish, and the inverse association with non-soy legumes, persisted in women but not in men.
Dairy products significantly increased the risk of gout in women and increased the risk nonsignificantly in men (P=0.04 for interaction).
A 4-year lag sensitivity analysis in 48,805 participants with 1,279 cases of incident gout found that the positive associations between total protein, red meat, poultry, fish, and shellfish with gout was largely unchanged.
During the two follow-ups, 9,317 people reported that they had been diagnosed with another arthritis. The significant positive association between intake of total protein, poultry, fish, and shellfish and incident gout remained after excluding these participants.
The inverse association with soy foods and legumes was attenuated to become nonsignificant, but in a multivariate-adjusted model with dietary variables, compared with the lowest quartile intake, the HR of the higher three quartiles combined was 0.89 (95% CI 0.78-1.01) for soy food and 0.92 (95% CI 0.80-1.04) for legumes.
The study had limitations including self-reported gout. Also, information on gout treatment was not collected. Other limitations include the possible misclassification of dietary intake from the use of a food frequency questionnaire and the exclusion of people who did not participate in the follow-up interviews and who were older.
Also, the Chinese diet differs from a Western diet, the authors pointed out, but added that "our findings from this population-based cohort of Chinese in Singapore provide evidence for dietary guidelines in the prevention of gout that are applicable to other Asian populations."
The study was supported by the NIH.Teng and co-authors disclosed no relevant relationships with industry.
- Reviewed by Robert Jasmer, MD Associate Clinical Professor of Medicine, University of California, San Francisco and Dorothy Caputo, MA, BSN, RN, Nurse Planner
New hope for Gout Sufferers

Media release from Northland DHB
Hope and treatment are available for the more than 6000 people* in
the Northland region who have gout, a potentially crippling form of
arthritis that can strike at any time.
Arthritis New Zealand is
launching a campaign this Friday – ‘Don’t get trapped by gout!’ – to
raise awareness about gout, and to encourage Kiwis who think they may
have the illness to see their GP, so it can be managed and treated. New
Zealand has one of the highest prevalence’s of gout worldwide.
Sandra Kirby from Arthritis New Zealand says gout is the second most
common form of arthritis in New Zealand, and one of the most painful.
“It’s
caused by too much uric acid in the blood and affects joints, causing
sudden attacks of pain, often coming on overnight. It can affect any
joint but initially it often affects the big toe or another part of the
foot. The skin over the joint may also become red and shiny.”
Ms
Kirby says there are a number of myths and misunderstandings about
gout, including that it is an ‘old man’s disease’, mainly affects the
wealthy and can’t be treated.
“In fact, while gout is more likely to occur in males and in Māori and Pacific people, it can strike at any time.”
She says the good news is gout can be managed, and while there is no cure, there is treatment to ease pain and other symptoms.
“This
campaign has a simple message – if you think you have gout, go and see
your GP, or contact Arthritis New Zealand – www.goutnz.org.nz or 0800
663 463.”
Former All Black and Hurricanes prop Neemia Tialata
knows first-hand how painful and debilitating gout can be, having been
diagnosed at the age 20 after a rugby game.
“I was in so much pain and couldn’t walk. I saw a doctor who diagnosed gout and put me on daily medicine straight away.
“I
couldn’t believe it at first. I didn’t know gout was a form of
arthritis, that someone my age could have it, or that Pacific Island and
Māori people, especially men, are more likely to get it.”
Now
aged 32, Neemia says taking his daily medication and moderating his diet
by limiting shellfish, beer and red wine, has allowed him to keep his
gout under control and continue his rugby career.
His advice to anyone who thinks they might have gout is to see their doctor.
“Don’t be shy or scared about it. See your GP so you can get the right medication and advice and stay on top of it.”
Things you probably didn’t know about gout
1. Gout is a form of arthritis – it’s the second most common form of arthritis in New Zealand.
2.
Gout is caused by too much uric acid in the blood. It’s normal and
healthy to have some uric acid in your body and most people get rid of
it through their urine.
3. High levels of uric acid can turn
into crystals that are very sharp, like needles, and make your joints
very painful. Gout often occurs in the big toe.
4. About 80
percent of the time high uric acid is caused by people’s genes, their
weight or kidney problems. About 20 percent is caused by food and drink –
things like meat, seafood, beer and fizzy drinks.
5. Gout is three times more common in men than women.
6. Many Māori and Pacific men are genetically more likely to get gout – it’s estimated up to 14 percent of Pacific men have it.
7. If you think you may have gout, go and see your GP or visit the Arthritis New Zealand Gout website.
8. Thankfully, gout can be easily managed – there are effective medicines available to treat it.
9.
You can help control gout by taking your gout medication every day –
even if you aren’t having a gout attack. Losing weight, eating healthy
food and staying away from alcohol and fizzy drinks can also help.
10. Former All Black and Hurricane prop Neemia Tialata has gout – and controls it with daily medication and diet.
11.
If you have gout, you’re in good company! Famous people who suffered
from gout include Sir Isaac Newton, Sir Laurence Olivier, Frederick the
Great and Leonardo da Vinci.
12. The ancient Greeks used to
treat gout attacks with a drug from the crocus lily bulb called
colchicine. Colchicine is still used as a gout medication today.
*Data from the Health Quality & Safety Commission’s Atlas of Healthcare Variation gout domain: http://www.hqsc.govt.nz/assets/Health-Quality-Evaluation/Atlas/goutSF/atlas.html)
Gout Risk Factors
From the Mayo Clinic
You're more likely to develop gout if you have high levels of uric acid in your body. Factors that increase the uric acid level in your body include:
- Diet. Eating a diet that's high in meat and seafood and high in beverages sweetened with fruit sugar (fructose) promotes higher levels of uric acid, which increases your risk of gout. Alcohol consumption, especially of beer, also increases the risk of gout.
- Obesity. If you are overweight, your body produces more uric acid and your kidneys have a more difficult time eliminating uric acid, which greatly increases your risk of gout.
- Medical conditions. Certain diseases and conditions make it more likely that you'll develop gout. These include untreated high blood pressure and chronic conditions such as diabetes, metabolic syndrome, and heart and kidney diseases.
- Certain medications. The use of thiazide diuretics — commonly used to treat hypertension — and low-dose aspirin also can increase uric acid levels. So can the use of anti-rejection drugs prescribed for people who have undergone an organ transplant.
- Family history of gout. If other members of your family have had gout, you're more likely to develop the disease.
- Age and sex. Gout occurs more often in men, primarily because women tend to have lower uric acid levels. After menopause, however, women's uric acid levels approach those of men. Men also are more likely to develop gout earlier — usually between the ages of 30 and 50 — whereas women generally develop signs and symptoms after menopause.
- Recent surgery or trauma. Experiencing recent surgery or trauma has been associated with an increased risk of developing gout.
Gout management best practices require getting around misconceptions

By: M. ALEXANDER OTTO, Family Practice News Digital Network
MAUI, HAWAII – Urate-lowering therapy doesn’t have to be suspended while gout patients are treated for acute attacks, according to rheumatologist Orrin Troum of Santa Monica, Calif.
In fact, there are arguments against it; stopping allopurinol or other urate-lowering therapies (ULTs) during an attack doesn’t seem to help, and there’s a chance that patients might have another attack when it’s reintroduced. Still, the practice persists despite evidence and recommendations to the contrary, Dr. Troum said at the 2015 Rheumatology Winter Clinical Symposium.
Gout is a curable or at least eminently manageable condition, but it remains a tricky problem to treat. Part of that is because referring physicians might be using an out-of-date playbook before sending patients for a rheumatology consult; another issue is that optimal care requires follow-up visits, which might not always be possible.
Gout management guidelines from the European League Against Rheumatism (Ann. Rheum. Dis. 2006;65:1312-24) and the American College of Rheumatology (Arthritis Care Res. 2012;64:1431-46) now largely concur on how best to handle the condition, which might help bring uniformity to gout management if their message filters through to other branches of medicine, said rheumatologist and copresenter Martin Bergman of the department of rheumatology at Drexel University in Philadelphia.
Another persistent misconception is that ULT can’t be started during an acute attack. “There are some very good studies showing” that it can so long as antiflare drugs are on board and patients follow up to check for hypersensitivity reactions and other potential ULT problems, said Dr. Bergman, also chief of rheumatology at Taylor Hospital in Ridley Park, Pa.
Starting low and going slow, a key concept with ULT, hasn’t fully taken hold outside the rheumatology community, either. With allopurinol, that means starting at 100 mg/day – and 50 mg/day in those with chronic kidney disease – then titrating up slowly over several follow-up visits to an effective serum uric acid (SUA)–lowering dose. The idea is to lower serum uric acid slowly, to avoid precipitating an acute attack.
Even so, patients are still sometimes started on 300 mg/day, and although more than half will need more than 300 mg/day to reach SUA targets, that dose is still sometimes considered to be the maximum allowable.
Overall, the consensus on both sides of the Atlantic is that gout patients need to have serum urate levels below 6 mg/dL, and below 5 mg/dL if they have tophi.
“So the next question is, ‘How low do you go?’ ” It’s recently been found that “lifelong maintenance on very low levels of uric acid might actually increase the risk of neurodegenerative diseases, such as Parkinson’s, multiple sclerosis, and dementia.” Uric acid is a strong antioxidant that, perhaps, has protective effects in the central nervous system, Dr. Troum said.
It might be best to go below 5 mg/dL in severe gout for only 3-5 years, then loosen the target to 5-6 mg/dL (Nat. Rev. Rheumatol. 2014;10:271-83), he added.
Among other recent developments, it’s now known that psoriasis and psoriatic arthritis substantially increase the risk of gout (Ann. Rheum. Dis. 2014 March 20 [doi:10.1136/annrheumdis-2014-205212]), so it’s important to check for gout crystals when aspirating inflamed joints in those conditions. It remains unclear, however, if psoriasis or gout should take precedence when crystals are found, Dr. Bergman said.
Also, it makes sense to screen patients for their HLA-B genotype. Carriers of the variant allele HLA-B*5801 are at high risk for severe cutaneous adverse reactions with allopurinol, so another ULT is probably a better option. The variant is most common in individuals of Korean, Han Chinese, or Thai descent (Clin. Pharmacol. Ther. 2013;93:153-8).
Dr. Troum is an adviser, consultant, speaker, or grant recipient for several companies, including AbbVie, Amgen, Bristol-Myers Squibb, Centocor, Novartis, Pfizer, and Roche. He holds shares in Theralogix. Dr. Bergman is an adviser, speaker, or consultant for several companies, as well, including AbbVie, Celgene, Amgen, and Roche. He holds shares in Bristol-Myers Squibb, Pfizer, and Johnson & Johnson.
Running to Live and Reduce Gout

Elloree Police Chief Preston Avinger has dropped from 272 to about 228 pounds over the past two years. He will compete in the Cooper River Bridge Run in Charleston on March 28, with all financial support he garners going to the Semper Fi Fund, which assists soldiers injured in combat after 9/11. Faced with gout, high blood pressure, diabetes and other health problems, Avinger adopted a healthier lifestyle and exercise regiment after realizing he had to make drastic changes in his life if he wanted to live.
By DWAUN SELLERS
T&D Correspondent
ELLOREE -- Preston Avinger, Elloree police chief, set out about two years ago to try to solve a case in which a life was in the balance -- his own life.His enemies were his poor diet and lack of exercise. Along the way, the evidence pointed to his ultimate demise if he failed to crack the case. He realized he had to shed the 100 pounds he'd gained over two decades and, in doing so, tackle the host of health issues he was facing because of his excessive weight. Avinger, 48, was born and reared in Santee. After high school, he enlisted in the Marine Corps Reserve while studying for his associate's degree at Orangeburg-Calhoun Technical College. In 1989, he transferred to active duty for four years, asking to be assigned to an infantry unit."My weight then was probably around 170," Avinger said. During this time, he dropped to 150 pounds as a result of the rigorous training, including running an average of 10 miles daily."When I got out of the Marine Corps (in 1993), I decided to keep my running up, and did it for probably the first year or two," he said. "The thing that really killed my running was going to the Criminal Justice Academy. They only run 30 minutes in the morning, and I was used to running an hour, an hour and a half every day. Going to class all day broke my routine. I got lazy."Avinger's new career in law enforcement meant working swing shifts and eating fast food on the run.He was diagnosed with high blood pressure."I really didn't consider myself overweight (at that point)," he said. "I was (weighing) in the 180s. I took a physical, and they told me my blood pressure was elevated and they wanted me to exercise and diet. But I didn't. I kept on working and doing what I was doing. My blood pressure got worse and worse until I was put on medication."Over time, Avinger's weight continued to increase and so did his physical ailments."In 1995, I started to get pains in my feet," he said. "I woke up one day and my big toe was swollen; I could hardly walk. I had no clue. I thought I was sleepwalking at night and jammed my toe. I didn't know what it was. Went to the doctor, and he told me it was gout."Gout occurs when the uric acid in the blood becomes so elevated it causes crystals to form in the blood, Avinger said. Once those crystals deposit in the joints, they grind in and cause inflammation and pain, causing the joints to swell, he said."The average person just gets it in their big toe," he said. "I started getting it to where I could hardly walk."The doctor told him gout was hereditary."My dad had it but he didn't start getting small attacks until his late 60s. But he's never had it like I've had it," Avinger said. "So here I am in my 20s and I'm getting gout. I wasn't in bad shape. I wasn't in great shape, but I was still doing some exercises -- still under 200 pounds."The inflammation, however, continued to cripple him."I started getting (gout) in other areas like my ankles, my elbows, fingers, knees, hip. One time, I was down for almost three weeks. Could hardly walk. I had to crawl to the bathroom. It was pretty bad," Avinger said.Medication provided only a temporary fix."I tried everything. Shots in the joints. Steroid shots," he said. "Over the years, they've come out with new medicines and they'd fast track me to get on (it), and it seems like it would get worse."His body began reacting adversely to some of the medications. In addition to gout and high blood pressure medication, Avinger was also being treated for diabetes and high cholesterol."Whenever my gout was bad and they'd give me that steroid shot, it would cause my diabetes to go completely out of control. And (the shot's effects) would last for a month to six weeks," Avinger said. "You can hardly walk, you don't feel good, your diabetes is messed up, your blood sugar is high and then I'd have to double or triple my medication (to balance it out). I was going through this crazy (cycle)."It was getting to the point where I didn't know what was going to happen. I was taken to the limit on my medication for blood pressure, taking four shots a day for diabetes and taking oral medication. And I was taking medication for my cholesterol, my triglycerides, and all of this was costing me so much money."Two years ago, Avinger saw a specialist at the Medical University of South Carolina about his gout. The physician told him there was only one more treatment they could try -- but it was life-threatening.The specialist said the new drug was for people who were completely disabled by gout. A number of patients had died from an allergic reaction to the drug, he told Avinger.Avinger was faced with this harsh reality, but he knew he had to make drastic changes in his life if he wanted to live. He said he started with a food diary, tracking every calorie he consumed. He then cut pork completely out of his diet."I haven't had a serious gout attack since (that day)," he said. "Within a few days, the pain was alleviated. That was two years ago."At that point, Avinger was tipping the scales at 270 pounds. His new commitment to a healthier lifestyle prompted him to make more changes. Last August, unable to run as he had 20 years ago, he began walking.The walking evolved into short jogs that led to longer jogs."I got all sorts of injuries," Avinger said. "My feet would hurt, my knees would hurt and I'd have to take a couple days off. But after the first couple of months of not giving up, things smoothed out."Avinger now runs three to four days a week, and on the days he's not running, he bikes it. Using an app on his phone, he tasked himself with running a 10K in January, "just to see if I could do it." He finished the 6.2 miles in an hour and 15 minutes.In addition to running and biking, Avinger uses an in-home treadmill on days when weather conditions prevent outdoor exercise.His new diet consists mainly of a protein shake in the morning, a veggie salad dressed with oil and vinegar for lunch and a portioned, controlled meal for dinner. He said he mostly drinks water now."It's been a process and it hasn't been easy," Avinger said. "The first couple of weeks the weight dropped off like water. I went from 272 to 250 pounds within a couple of weeks, but then it (plateaued). From then on, it's been hard going, but as long as I keep going, it's slowly coming off."He now weighs 228 pounds and his goal is to reduce to 170 by this time next year. At this weight, he believes he'll be able to regulate his blood pressure and further reduce the amount of medication he's on."I don't know what would have happened if I didn't have all these health issues," Avinger said. "I don't know what kind of weight I'd be at. I'd look in the mirror and say, 'Man, I look bad,' but then it's nothing really motivating you besides the way you look. That's vanity."But when the doctor says, 'You're going to die if you don't do something,' that's not fair to your children and the people who love you. You've got other people to consider when you're doing something to yourself that can kill you in the short-term."With his fitness routine firmly in place, Avinger is looking to cross off new benchmarks. The first will be participating in the Cooper River Bridge Run on Saturday, March 28, in Mt. Pleasant/Charleston. He's dedicating this run, and all financial support he garners, to the Semper Fi Fund, which assists soldiers who were injured in combat after 9/11."It's an organization that I've donated to personally," Avinger said. His fundraising goal was $700, but after surpassing that, he's raised it to $1,000."It makes you feel better when you've got goals to look forward to instead of just trudging along thinking you're just losing weight," he said.Once he's got the Cooper River Bridge 10K under his ever-tightening belt, Avinger said he plans to run the Marine Corps marathon (26 miles) next year in memory of his two childhood best friends he lost to a rare form of leukemia.Avinger hopes his weight loss journey inspires others as much as it has reignited his own desire for a healthier lifestyle.To donate to Avinger's Cooper River Bridge Run, visit https://2015-cooper-river-bridge run.everydayhero.com/us/preston. Contact the writer: [email protected].
When in gout, see a doctor
by VERONICA PULUMBARIT
…and the doctor you should see is a rheumatologist.
Admittedly, that word is quite a mouthful. A trick for remembering that word: “rayuma” (Tagalog for arthritis) equals “rheumatologist.”
A rheumatologist treats people with arthritis (inflammation of the joints) or rheumatic diseases such as lupus and uncommon illnesses, including Ankylosing Spondylitis, and Sjogren's Syndrome.
Out of all these diseases, the Philippine Rheumatology Association (PRA) chose to launch a year-long campaign for awareness about gout.
The PRA defines gout as “an episodic, severely painful form of inflammatory arthritis due to increased uric acid.”
The disease affects 1.6 percent of the national population, meaning that out of 100 million Filipinos, about 1.6 million are gout sufferers.
Gout primarily affects men in their 20s and 30s, but there are women victims as well. According to the Mayo Clinic, women become "increasingly susceptible" to it after menopause.
During the 21st annual meeting of the PRA, Dr. Eric Jason Amante, PRA president, said the mismanagement of gout as a disease is becoming prevalent in the Philippines.
'Extreme' pain
If left untreated, “gout becomes more severe and attacks become more frequent,” said the PRA. “During gout attacks, pain is extreme. Even lightly touching affected joints can be intolerable.”
As the flyers, posters, and stickers for the campaign say, “There’s pain, then there’s gout pain.”
Mary Buenaventura, president and CEO of the Y&R PR group that prepared the materials for the campaign said they asked several gout sufferers to describe the pain they experienced.
Those who had gout said the pain is severe and unlike any they have experienced, Buenaventura said.
“Gout pain is a unique kind of pain,” she said, adding that “there are no words to describe it.”
In the video prepared for the gout awareness campaign, Steve Badiola, the 32-year-old singer of Typecast band, described gout as “sobrang sakit, mapapamura ka.”
PRA emphasizes: See a doctor
Amante said that often, when people experience gout symptoms, they tend to self-medicate.
He said some people seek advice on gout relief from family, friends, co-workers but not from rheumatologists who are trained to handle this disease.
Noting that most of the people affected by gout are in their 20s to 40s and are part of the working sector, Amante said the disease has a financial toll. Loss of income, loss of productivity, and absenteeism are some of the non-health problems associated with gout, he said.
Gout “leads to missed days at work, anger, and overall poor quality of life,” said the group.
Furthermore, if left untreated, gout can lead to kidney stones, joint erosions, deformities, and even kidney failure.
According to Amante, sometimes when gout sufferers first come to rheumatologists for treatment, it’s often too late and they are already in wheelchairs.
He stressed that people need to realize that gout can be managed just by visiting rheumatologists who can prescribe them the right medicine.
He added that the majority of those who have gout are in the low-income group, which is why they tend to self-medicate or take no medication at all.
Asked if the PRA will have a program to help gout sufferers who are less privileged, Amante said their current campaign is mainly for informational purposes but they will come up with a project for those who cannot afford medical treatment. — BM, GMA News
Study states - Gout Reduce Risks of Alzheimer’s Disease
By Saranya Palanisamy [email protected] Mar 17, 2015 05:55 AM EDT
People
experiencing gout could be at a lower risk of Alzheimer's disease says a
recent study published in the Annals of the Rheumatic Diseases. The
study demonstrated a unique association between gout, a complex form of
arthritis, and Alzheimer's disease, a chronic degenerative dementia.
According to Delaware Online,
about 24 percent of people that experienced gout had reduced risk of
Alzheimer's disease reports scientists at Massachusetts General Hospital
and Boston University Medical Center. Their study involves 59,224
people with gout and 238,805 people without gout aged around 65, with
men accounting to 71 percent of the study population.
Gout is characterized by sudden, severe attacks of pain, redness and
tenderness in joints, often the joint at the base of the big toe and is
much common in men, and largely in women post menopause. A burning
sensation of the big toe is usually experienced at nights. In severe
cases, even the bed sheet on the toe would feel heavy, according to Mayo Clinic.
Alzheimer's disease, on the other hand, is a progressive dementia
often seen in elderly people characterized by loss of memory and other
important mental functions. The brain cells degenerate themselves and
die slowly and steadily resulting in loss of intellectual and social
skills. A combination of genetic, lifestyle, and environmental factors
are believed to cause this degenerative dementia, says the Mayo Clinic.
Though the mechanism of the disease is quite known there is no cure
found so far.
Gout is caused as a result of increased levels of uric acid in blood
and is associated with issues relating to kidney stones and
cardiovascular problems wherein a positive association of gout against
neurodegenerative diseases and Parkinson's disease were also reported
lately.
The anti-oxidant properties of uric acid have neuro-protective
benefits, says the researchers. Uric acid helps in repairing the damage
caused by the free radicals to the cells and DNA by scavenging free
radicals, atoms or molecules with unpaired electrons that combine easily
with other molecules, says the Washington Post.
Hyon Choi, a professor of Medicine at Harvard Medical School and
leader of the new research, said that the study doesn't confidently
claim that uric acid protects the brain since a lot of research and
years of work are necessary to come to a conclusion on the subject.
"If this happens to be true," he said, "then we are talking about
potentially major implications. But, again, (it is) still speculative at
this point" noted the researcher, according to the Washington Post.
Gout Treatment can be more effective by Genetic testing

From Arthritis Research UK.
The treatment of gout could be made more efficient and effective through the use of genetic screening techniques, according to a new study from South Korea.
Led by Chonnam National University Medical School & Hospital, the research project aimed to evaluate the cost-effectiveness of HLA–B5801 genotyping for the treatment of gout in Korean patients with chronic renal insufficiency.
Currently, the drug allopurinol is a common treatment for gout, but the therapy can in rare cases be associated with severe cutaneous adverse reactions (SCARs) that cause high rates of morbidity and mortality.
Past studies have shown that the HLA–B5801 allele and renal impairment are strongly associated with SCARs, leading to the hypothesis that HLA–B5801 genotype testing of gout patients at high risk for SCARs should be conducted prior to treatment with allopurinol.
For this new research, a decision analytical model was employed over a 12-month period to compare the cost and outcomes of treatment informed by HLA–B5801 genotyping with that of a conventional treatment strategy. Direct medical costs were obtained from real patients with SCARs from two tertiary hospitals.
According to results published in the medical journal Arthritis Care & Research, the total expected cost for the conventional strategy was $1,193 (£791.84), but dropped to $1,055 (£700.23) when the gene testing was employed.
Moreover, the probability of continuation of gout treatment without SCARs was 100 per cent in the HLA–B5801 genotyping cohort, compared to 97.8 per cent in the control group.
The researchers concluded: "Our model suggests that gout treatment informed by HLA–B5801 genotyping is less costly and more effective than treatment without genotyping, and HLA–B5801 genotyping could considerably reduce the occurrence of allopurinol-induced SCARs and related deaths."
A spokesman for Arthritis Research UK, which funds research into gout, commented: "Genotyping of gout patients is not widely performed and currently has little clinical application in the UK. The most important aspect of gout treatment is making sure that both people with gout and their doctors are aware of the effectiveness that lifestyle changes and dose escalation of drugs such as allopurinol can make, as these factors can reduce uric acid levels and hence attacks of gout." - See more at: http://www.arthritisresearchuk.org/news/general-news/genetic-testing-can-increase-effectiveness-of-gout-therapy.aspx#sthash.7NYWheDE.dpuf
Gout discovery by Japanese
Researchers have identified a genetic predisposition for gout that puts certain people at a greater risk of contracting the painful condition. Analyses of genes of 1,600 Japanese male gout patients and 1,300 healthy Japanese men found a heightened risk among people with gene variations that weaken the ability of the kidney and intestinal tract to release uric acid, the researchers said. The finding was announced in the online version of British journal Annals of the Rheumatic Diseases. The team included Hirotaka Matsuo, a lecturer at the National Defense Medical College, Ken Yamamoto, a professor at Kurume University, and Hirofumi Nakaoka, a researcher at the National Institute of Genetics. It may become possible develop personalized treatment for gout patients depending on analysis of DNA from a blood sample, Matsuo said. Gout, which causes strong pain in joints, occurs when uric acid builds up in the blood. Uric acid is generated as a result of cellular metabolism and is produced from purines from ingested foods and drinks. Gout is also known to increase the risks of cerebral vessel and cardiac diseases. Recent studies have found that gout results not only from eating habits and obesity but also from deterioration in the functions to release uric acid from the body. In 2009, Matsuo and others discovered a gene called ABCG2, which plays an important role in the release of uric acid through the intestinal tract. The latest research found that problems with this gene boost the risk of gout three- to fourfold. Similarly, the gout risk doubles if there are problems with another gene, SLC2A9, tied to the release of uric acid through the kidney, the team reported.
Acute gout attacks experienced most commonly at night
New York, Dec 14: A recent study has revealed that the risk of acute gout attacks is more than two times higher during the night or early morning hours than it is in the daytime. The study was published in Arthritis & Rheumatology, a journal of the American College of Rheumatology (ACR).
Here’ what you should know about gout
The nocturnal attacks persist
even among those who did not consume alcohol and had a low amount of
purine intake during the 24 hours prior to the gout attack. The body
produces uric acid from the process of breaking down purines – natural
substances in cells in the body and in most foods. High purine levels
are found in organ meat, seafood and alcohol (yeast).
Acute gout flares are triggered by the crystallisation of uric acid within the joints, and experts believe these flares are ‘among the most painful events experienced by humans’. ‘It is speculated that lower body temperature, night-time dehydration, or a nocturnal dip of cortisol levels may contribute to the risk of gout attacks at night,’ said lead author Hyon Choi of the Massachusetts General Hospital and the Harvard Medical School in the US.
How was the study conducted?
The research team recruited 724 gout patients, who were followed for
one year via the internet. Findings indicate that participants
experienced 1,433 gout attacks – 733 in the overnight hours (midnight to
7.59 a.m.), 310 in the daytime (8.00 a.m. to 2.59 p.m.), and 390 in the
evening (3.00 p.m. to 11.59 p.m.) during the one-year study period.
What did the results indicate?
The risk of a gout flare was 2.4 times higher
overnight and 1.3 times higher in the evening compared to daytime
hours. ‘As a result of our study, prophylactic measures that prevent
gout flares, especially at night, may be more effective,’ the
researchers said. Furthermore, researchers found that this risk
persisted even among those with no alcohol intake and low purine intake
during the 24 hours prior to the gout attack.
With inputs from IANS

Children born by C-section face higher chronic illness risk.
Copenhagen Press
Findings based on 2 million children born between 1973 and 2012
The risk of getting asthma is higher when born by C-section, as are immune defects and juvenile gout
People born by Caesarean section are more susceptible to a number of chronic illnesses – including asthma, allergies, gout, intestinal illness and leukaemia – than people who are born vaginally, according to a new massive Danish study.
The study, which has just be published in the scientific periodical Pediatrics, has researched the link between C-sections and immunological illnesses in 2 million Danish children born over a 35-year period from 1973 to 2012.
”We show for the first time that C-sections can be a common risk factor for several immunological illness – both child illnesses like asthma and allergy, but also illnesses that only develop later in life,” Hans Bisgaard, a professor of child asthma at the Danish Child Asthma Centre in Copenhagen, told science site Videnskab.dk
The research revealed that children born via C-section are more often hospitalised because of asthma, juvenile gout, inflammatory intestinal illness, immune defects, leukaemia or connective tissue diseases during their lives than their vaginally-born peers.
Not a direct link
More specifically, the risk of getting asthma is about 20 percent higher
when born by C-section. Additionally, the risk of immune defects is
about 40 percent higher and the risk of juvenile gout is about 10
percent higher.
But the research doesn't prove that a C-section is the reason for developing illnesses later in life as the study doesn't show a direct link. There could be a number of reasons why C-section children are more often ill, Bisgaard argues.
Previous studies have shown that C-section children have are at greater risk than others at becoming asthmatics, allergics and diabetics, but it's the first time that a single study has found a link between C-sections and a number of immunological illnesses.
”We know there are a number of genes that are common for several of these immunological illnesses, and the C-section can be one of several factors that activate the said genes so that people become ill,” Bisgaard said.
Gout Game Educates UNMC Students, Future Physicians on Poorly Managed Disease
By Staff Editor
(HealthNewsDigest.com) - As part of the push to develop new and better ways of teaching, second-year medical students at the University of Nebraska Medical Center are playing a video game to learn about gout, a painful disease that is poorly managed.
"We found about half of the students don't like sitting in lectures," said Amy Cannella, M.D., assistant professor of internal medicine at UNMC. "They like to view them online at double speed or half speed. They also study outside of the classroom then come together in small groups and have discussions. This is similar to the teaching trend called ‘flipped classroom.' "
The "retro" video game was developed through a grant collaboration with the University of Nebraska at Omaha. The idea is to engage students in a fun way to better help them understand and more effectively treat gout. Currently the game is optional for students.
"Gout is a bad disease and it's terribly managed. It affects 4 to 5 percent of the population," Dr. Cannella said. "If we can impress basic principles of gout management on students who may become primary care practitioners, they can make a difference with this disease. Many primary care practitioners take care of gout patients without specialty training."
The faculty polled students on what they thought about the game. Though it didn't show the learning outcomes were any better, students said they enjoyed learning the subject material more than in a traditional format.
In the game, students and their patients ride a dune buggy to navigate various landscapes through different aspects of the disease, symptoms and treatment.
"There are high stakes," Dr. Cannella said. "Players must avoid hazards such as alcohol, which increase their risk of gout, and correctly answer questions about the disease."
Tate Johnson, UNMC medical student, said he enjoyed the game. "Since it's a unique and fun learning tool, it makes it easier to think back to the game and recall the information I learned. I think providing simple alternative memory tools like this is a really great way to emphasize important information."
Anyone interested in learning about gout can download and play the game athttp://gout.ist.unomaha.edu/
###
For advertising/promotion contact Mike McCurdy at 877-634-9180 or email at: [email protected] - We have over 7,000 journalists as subscribers.
Comorbidities Frequent in Gout Patients
By Wayne Kuznar , Contributing Writer, MedPage Today
save|AA
Comorbidities are common in patients with gout at diagnosis and are even likelier following the diagnosis, according to a case control study by authors from the U.K. and Taiwan.
"This study suggests that a thorough search for a broad range of comorbidity and subsequent vigilant observation should be considered for all patients with gout from the date of first diagnosis," they wrote in Annals of the Rheumatic Diseases.
The case control study was conducted within the Clinical Practice Research Data-link, a U.K. database containing medical records of about 12 million individuals. From this database, 39,111 patients (72.5% men; mean age, 62.2 years) with incident gout were identified. Controls were matched individuals without gout identified at random from the same database. Comorbidities were assessed 10 years prior to diagnosis, 1 year prior to diagnosis, and from diagnosis to the occurrence of a comorbidity, death, or end of the study. The cumulative probability of comorbidity was estimated at the time of diagnosis (index date) and at 1 year, 2 years, 5 years, and 10 years following diagnosis.
At the time of diagnosis, significantly more people with incident gout had at least one comorbidity in the Charlson index compared with controls (32.25% versus 27.95%; P<0.001). Retrospective observation showed that cardiovascular and genitourinary diseases were associated with a higher risk for incident gout. The highest risks were for renal diseases, with an odds ratio (OR) of 5.96 and congestive heart disease (OR 4.37). In adjusted models in the 10-year and 1-year periods prior to diagnosis, hyperlipidemia (OR 1.71), hypothyroidism (OR 1.50), anemia (OR 1.40), psoriasis (OR 1.32), chronic pulmonary diseases (OR 1.30), osteoarthritis (OR 1.27), and depression (OR 1.09) were positively associated with incident gout.
Development of a first comorbidity was significantly faster in patients with incident gout. The median time to a first comorbidity was 43 months (95% CI 41-45 months) in patients with incident gout and 111 months (95% CI 108-115 months) in controls (P<0.001). A first comorbidity occurred in 42.09% of the group with incident gout versus 30.78% of the controls at 1 year post index, 45.39% versus 33.32% at 2 years, 53.99% versus 40.92% at 5 years, and 66.28% versus 51.51% at 10 years.
The cumulative probability of any increase in the Charlson index after diagnosis was significantly greater in patients with gout than in controls at all time points after diagnosis (P<0.001).
Gout was associated with an adjusted hazard ratio (HR) of 1.41 (95% CI 1.34-1.48) for having a Charlson index ≥1. The risk of an incident cardiovascular, genitourinary, metabolic/endocrine, and musculoskeletal/connective tissue disease comorbidity was higher in patients with gout, including triple the risk of incident renal disease (HR 3.18, 95% CI 2.88-3.50). Risks of liver diseases, hemiplegia, depression, anemia, and psoriasis were also higher in patients with gout.
Mortality at 5 years and 10 years after the index date was significantly higher (P<0.001) in patients with gout compared with matched controls: 14.43% versus 11.14% at 5 years and 26.98% versus 21.66% at 10 years. After adjustment for potential confounders, gout was associated with a HR of 1.13 (95% CI 1.08-1.18) for all-cause mortality (P<0.001).
Because some of the comorbidities, such as hypothyroidism and anemia, found to be associated with gout are not included in gout patient management guidelines, "this study supports the case for a comprehensive investigation for comorbidities, including but not limited to 'checklists,' as an integral part of initial assessment for patients with gout at diagnosis," according to the authors.
Limitations include potential misclassification of gout and comorbidities. In addition, all potential risk factors for gouty arthritis are not recorded in the database and therefore could not be adjusted for.
BMI & GOUT

Gout linked to BMI
The Greater the weight you carry , the greater your chance of developing gout. A new review has correlated body mass index with gout and found each five-unit increment on the BMI scale is associated with a 55 per cent increased relative risk of gout. The review, of several studies, involved a total of 28,000 cases of gout in a population of 216,000 participants.
The results, published in the European Journal of Nutrition, suggest the link between gout and BMI exists independently of other established risk factors for gout, including cholesterol levels, alcohol intake, diuretic use, renal insufficiency, and consumption of meat, seafood and certain fruit and vegetables. It suggests greater amounts of body fat may increase the risk of gout by increasing uric acid levels in the blood. This is particularly so for abdominal fat - such as a beer gut.
The Australian Financial Review
This is the latest Gout News from around the world.
It is critical that you keep up to date with the latest Gout News and information. New Gout drugs and Gout Treatments are occurring every week. Some good , some bad, some with side effects some without.
Gout Risk reduced by Smoking

Ok, I have now heard it all about Gout cures.
Can smoking cigarettes, actually reduce GOUT?
Well according to a new study published online in Rheumatology.
Weiqi Wang, PhD, and Eswar Krishnan, MD, MPH, of Stanford University School of Medicine in Palo Alto, Calif., analyzed 54-year follow-up data (1948-2002) for 2,279 men and 2,785 women who were gout-free at their first assessment as part of the Framingham Heart Study.
The researchers identified 399 incident cases of gout (249 men and 150 women) over 151,058 person-years of observation. In multivariable analyses, cigarette smoking was associated with a 24% decreased risk of incident gout overall, a 32% decreased risk among men, and an 8% decreased risk among women, after adjusting for age, body mass index, alcohol intake, diabetes, hypertension, kidney disease, Drs. Wang and Krishnan reported.
So get another cancer stick into you, to reduce your gout today.
Unfortunately there is a far worse side effect of this gout cure.
Diabetes and gout could be linked

FRIDAY, Oct. 3, 2014 (HealthDay News) -- Gout, a form of inflammatory arthritis, appears to increase the risk of type 2 diabetes, especially in women, a new study finds.
Researchers followed more than 35,000 gout sufferers in the United Kingdom and found that women with gout were 71 percent more likely to develop diabetes compared with people without gout. For men, the increased risk was 22 percent.
"Gout seems to be contributing to the risk of diabetes independently of other diabetes risk factors, such as obesity," said lead researcher Dr. Hyon Choi, from the division of rheumatology, allergy, and immunology at Massachusetts General Hospital in Boston.
Gout causes intense pain and swelling in single joints, most often the feet, especially the joint at the base of the big toe. More than 3 million Americans suffer from the condition, men more often than women, according to the American College of Rheumatology.
People with gout have excess uric acid in the body, which forms needle-like crystals that lodge in the joints.
Diabetes, characterized by high blood sugar levels, can lead to kidney damage, heart disease and limb amputations over time. Clarifying its relationship to gout "is essential," the study authors said.
However, while the current research suggests gout raises the risk of diabetes, the study can't prove it. "The association is clearly there, but why that is so isn't known," Choi said.
Choi speculates that ongoing, low-level inflammation from gout may increase the risk for diabetes. Other risk factors shared by both diseases -- high cholesterol and high blood pressure, for example -- might also increase the risk, he said.
The researchers used data from health records on adult patients from January 1995 to May 2010. They zeroed in on about 35,000 people with newly diagnosed gout and compared them with more than 137,000 people without the condition.
To isolate the relationship between gout and diabetes, the investigators took age, sex and especially weight into account, because obesity is a risk factor for both gout and type 2 diabetes.
The study, published online Oct. 2 in the Annals of the Rheumatic Diseases, found that almost three-quarters of the new cases of gout were among men with an average age of 61. Among women with new cases of gout, the average age was 68.
The odds of developing diabetes alongside gout was much more likely for women, the researchers found. Choi said the absolute risk of a woman with gout developing diabetes is about 5 percent, and for a man it's about 3 percent.
People with gout tended to drink more alcohol, saw their doctor more often, had more medical problems, and took steroids and diuretics more often than those who did not have gout, the study authors noted.
Treatments for gout are available and are tailored individually.
Choi said the best way to reduce the risk of developing gout or diabetes is to control risk factors, such as blood pressure, cholesterol and weight.
Dr. Spyros Mezitis, an endocrinologist at Lenox Hill Hospital in New York City, said this study may make doctors more aware of the association between gout and diabetes.
"The question for doctors is whether people with gout should be tested for diabetes and people with diabetes tested for gout," Mezitis said.
"What this study tells us is that if the patient has gout, you have to be thinking that the patient is at increased risk for diabetes," he said. This may be independent of other factors normally associated with diabetes, such as obesity and high blood pressure, he added.
New results with testing of AstraZeneca’s Gout Drug
AstraZeneca announced positive top-line results from CLEAR1, CLEAR2 and CRYSTAL, the pivotal Phase 3 clinical trials investigating the potential of lesinurad, a selective uric acid re-absorption inhibitor (SURI), as a combination therapy for the treatment of patients with symptomatic gout. Lesinurad is an investigational agent that inhibits the URAT1 transporter, increasing uric acid excretion and thereby lowering serum uric acid (sUA).
CLEAR1 and CLEAR2 studied lesinurad (200mg and 400mg once daily) in combination with the xanthine oxidase (XO) inhibitor allopurinol, in symptomatic gout patients not achieving target sUA levels on their current allopurinol dose. CRYSTAL studied lesinurad (200mg and 400mg once daily) in combination with the XO inhibitor febuxostat (80mg once daily) in gout patients with tophi (visible nodules of uric acid crystals that are deposited in joints and skin).
In the CLEAR1 and CLEAR2 trials, both lesinurad 200mg and 400mg in combination with allopurinol met the primary endpoint, with a statistically significant higher proportion of patients reaching the target sUA goal of <6.0mg/dL at month 6 compared to allopurinol alone (p<0.0001).
In the CRYSTAL trial, lesinurad 400mg in combination with febuxostat met the primary endpoint, with a statistically significant higher proportion of patients reaching the target sUA goal of <5.0mg/dL at month 6 compared to febuxostat alone (p<0.0001). Although lesinurad 200mg did not achieve statistical significance at month 6 (p=0.13), this dose in combination with febuxostat, was superior to placebo plus febuxostat at all other time points (measured at months 1 to 5, 8, 10 and 12; nominal p<0.05).
The three most commonly reported adverse events across the CLEAR1 and CLEAR2 trials for patients receiving lesinurad in combination with allopurinol were upper respiratory tract infection, nasopharyngitis and back pain. In CRYSTAL, the three most commonly reported adverse events for patients receiving lesinurad in combination with febuxostat were nasopharyngitis, arthralgia and upper respiratory tract infection.
The incidence of renal-related adverse events (including serious events) and incidence of kidney stones with lesinurad 200mg plus XO inhibitor was comparable to placebo plus XO inhibitor. The incidence of renal-related adverse events and kidney stones was higher with lesinurad 400mg plus XO inhibitor. A full assessment of the safety and tolerability findings of all three studies is ongoing.
“Gout is a serious, chronic and debilitating inflammatory disease. There is a significant unmet need, with 40 to 70% of gout patients not reaching target levels of serum uric acid with the current standard of care,” said Briggs Morrison, Executive Vice President, Global Medicines Development and Chief Medical Officer. “We are encouraged by our initial review of the top-line results from the CLEAR1, CLEAR2 and CRYSTAL studies which provide important new information on the efficacy and safety of lesinurad in combination with febuxostat and allopurinol. These data indicate that combination therapy with lesinurad may be a potential treatment option for gout patients.”
CLEAR1, CLEAR2 and CRYSTAL were conducted by Ardea Biosciences, a wholly-owned subsidiary of AstraZeneca. Results from these Phase 3 clinical trials will be submitted to a scientific meeting later in 2014. The company is proceeding with preparation of regulatory submissions for lesinurad (200mg) combination therapy.
Date: August 13, 2014
Source: AstraZeneca
Gout & Uric Acid Education Society Introduces New Spanish-Language Patient Resources
Gout & Uric Acid Education Society Introduces New Spanish-Language Patient Resources
Published: August 13, 2014 11:01 AM
PRNewswire
PITTSBURGH, Aug. 13, 2014 /PRNewswire/ -- As the most common form of inflammatory arthritis today, gout is growing in epidemic proportions in the United States. With prevalence of comorbid health issues - including diabetes, high blood pressure and obesity - also on the rise, Hispanic Americans face even greater risks for developing gout.
http://photos.prnewswire.com/prnvar/20140811/135196
To help raise gout awareness and encourage proper diagnosis and management among at-risk Hispanic populations, the Gout & Uric Acid Education Society (GUAES) is expanding the availability of its Spanish-language patient resources.
An infographic featuring quick facts about gout and treatment options - which can double as a poster for medical professionals to place in waiting or exam rooms - and six patient fact sheets are now available in both English and Spanish through GoutEducation.org. Fact sheet topics include:
"The Hispanic population is not only growing in size, but also continues to represent a large and growing portion of gout sufferers," said N. Lawrence Edwards, M.D., Professor of Medicine, Rheumatology and Clinical Immunology, University of Florida, and Chairman and CEO of GUAES. "Recognizing that more than three out of four Hispanic Americans speak at least some Spanish, we are pleased to introduce new Spanish-language gout resources and hope to continue to expand our offerings in the future."
A Spanish version of the popular "Take a Stand on Gout" patient brochure is also available through GoutEducation.org. Printed copies of the brochure and infographic/poster can be ordered free-of-charge by patients and medical professionals through the website, or by contacting [email protected].
About the Gout & Uric Acid Education Society
The Gout & Uric Acid Education Society (GUAES) is a nonprofit organization of health care professionals dedicated to educating the public and health care community about gout - the most common form of inflammatory arthritis - and the related consequences of hyperuricemia. With the aim of improving the quality of care and minimizing the burden of gout, GUAES offers complimentary resources for both the general public and medical professionals at gouteducation.org. Twitter: @GoutEducation Facebook: Gout Education
Photo - http://photos.prnewswire.com/prnh/20140811/135196
Doctors chase cure for diabetic kidney disease in cheap pill for gout
Paul Wild has been a reliable research volunteer at the University of Minnesota for 20 years, participating in two landmark studies that changed the standard of care for diabetes, a disease that afflicts more than 24 million Americans.
“Looking back, it was probably the best thing I ever did,” said the 61-year-old Mendota Heights dentist.
Now, Wild is among 480 patients being recruited for a $24 million, 3½-year test to see whether a medication that has been used routinely to prevent gout can delay the onset of potentially fatal kidney disease in patients with Type 1 diabetes.
If the study succeeds, the medication, called allopurinol, could be to diabetic kidney disease what baby aspirin is to heart attacks, said Dr. Luiza Caramori, an endocrinologist helping to oversee the study at the U. The drug could delay the need for dialysis and kidney transplants by eight to 10 years, she said, saving thousands of lives and tens of millions of dollars in medical spending.
Diabetes has reached epidemic proportions in the United States, with rates increasing so fast that researchers predict 1 in 3 Americans born after 2000 could develop either Type 1 or Type 2. As many as 30 percent of diabetics will develop serious kidney disease within 10 to 20 years of their diagnosis, making it the leading cause of kidney failure in the United States. And because the waiting list for a kidney is so long, hundreds of patients die each year waiting for a transplant.
While the U study is limited to subjects with Type 1 diabetes, Caramori said positive findings will likely benefit the far more common Type 2 diabetics, as well.
“It’s amazing that in the past 20 years we’ve basically made no progress in delaying kidney disease in patients with diabetes,” she said. “It’s also disappointing and scary, because the rates of complications are quite high in these patients.”
Type 1 diabetes occurs when the immune system destroys the body’s ability to produce insulin. It affects fewer than 1 in 10 diabetics. The much more common Type 2 often results from genetic predisposition, coupled with obesity and lifestyle factors, leading initially to resistance to the body’s own insulin.
The U is one of seven U.S. sites and two international locations recruiting participants for the study, which is being led by Dr. Michael Mauer, a professor of pediatrics and medicine at the U’s medical school, and Dr. Alessandro Doria, an epidemiologist at Joslin Diabetes Center and associate professor at Harvard Medical School.
If allopurinol works as expected, it could become the standard treatment for treating diabetic kidney complications, Doria said in comments released last year.
Study seeking volunteers
Results from three small preliminary studies indicate that allopurinol shows real promise. It suppresses the production of an enzyme, xanthine oxidase, a result of metabolic activity, which can lead to excess acid in the urine. The World Health Organization lists it as an essential medicine for health systems.
It’s also cheap and has been used in the Untied States for nearly 50 years to prevent gout flare-ups.
The study seeks volunteers between 18 and 70 who’ve been diagnosed with Type 1 diabetes for at least eight years and who are concerned about possible kidney disease.
Although allopurinol is generally safe, researchers will screen study applicants for possible drug interactions and for a genetic profile that puts some at risk for a rare, serious skin disease.
The study will assign subjects randomly to two equal groups. They will get either allopurinol or a placebo — neither the patients nor their doctors will know which — and they’ll have to visit a study center or a site working remotely with the centers 17 times over three years for a variety of procedures and tests.
The U is one of nine institutions known as the Preventing Early Renal Function Loss in Diabetes (PERL) Consortium, which received the $24.3 million grant from the National Institute of Diabetes and Digestive and Kidney Diseases, a division of the National Institutes of Health (NIH). The nonprofit Juvenile Diabetes Research Foundation also is contributing to the PERL study.
Caramori said that leading diabetic researchers are involved and that they have big hopes for it.
Diabetics account for about 45 percent of people with end-stage kidney disease. Caramori said the survival rate, once they enter dialysis, is very low.
“So there’s a big fight trying to bring funds to diabetes research. There’s a lot of money allocated to cancer that can benefit, of course, many patients. But even more funds are allocated to AIDS, for example, where the fraction of the population that’s affected is much smaller,” she said. Though both diseases are important, by comparison, she said, “We are not doing well in terms of spending money in diabetes research.”
The allopurinol study is the only kidney disease trial and the only Type 1 diabetes trial that NIH funded this year.
Yet it’s not easy to find Type 1 diabetics who meet the study’s design criteria. Each study center is seeking 50 to 55 participants. HealthPartners, Hennepin County Medical Center and Essentia Health in Duluth are helping to recruit patients for the U center.
Of those interviewed as of July 7, 119 have gone through initial lab tests, including 14 at the U. Just 36 volunteers were cleared for additional tests.
Caramori said that recruitment is running well behind schedule and that the NIH extended the recruitment deadline to August 2015. Even so, she said. “If we are successful in recruiting these people, I think it’s very unlikely we are going to have a negative study.”
Dan Browning • 612-673-4493
Eating
soybean does not increase risk of gout
Eating soybeans will not increase the risk of gout, recent studies shows.
This belies widely-held public perception that eating soybeans can increase the risk of gout and can potentially trigger acute attacks for those already suffering from the disease. Most people believed this because beans are high in protein, concluding that consumption of high protein leads to high uric acid in the blood leading to gout
“This is not true as revealed by numerous scientific studies,” said Elmer E. Enicola, researcher from the Institute of Plant Breeding, University of the Philippines Los Baños (IPB-UPLB) in a seminar on soybeans organized by the Bureau of Agricultural Research (BAR) on 29 January 2014.
Enicola is not a medical practitioner and, as mentioned earlier in his presentation, the seminar aims mainly to inform the public by presenting the latest studies on soybean consumption. “I’m very interested in this topic since conventional wisdom can limit bean consumption in the country,” he added. He presented “Soybeans and Gout” as a public seminar to correct one of the most known anecdotes attributed to eating soybean and soy-based foods.
He described how gout develops in an individual which is likely to occur when there is excess uric acid in the blood. The uric acid builds up in the fluid around the joints leading to the formation of uric acid crystals which may cause the joint to swell and become inflamed. Gout is also known as “podagra” when it involves the big toe. Enicola discussed that gout can be acute or chronic. “It’s acute if only one or a few joints are affected, mostly like it’s either the big toe, knee or ankle joints. It becomes chronic when there are repeated episodes of pain and inflammation and that more than one joint is affected leading to damage and loss of joint motion,” Enicola said.
In the presentation, he explained how gout may be a consequence of high uric acid in the blood. Uric acid is the waste product from the metabolism of purines. What then are purines? Where do they come from?
“Some purines are made by the body itself since purines are part of the chemistry of the human body. But aside from that, purines can also come from the food we eat,” Enicola said. Among the foods that were categorized with high levels of purines and are best to avoid are: liver, kidney, anchovies, sardines, mussels, bacon, scallops, and beer.
Purines from the body and those from the food that we consume form the uric acid in the blood. This eventually builds up in the joints only if the body cannot keep up with excreting out the uric acid. “But this does not immediately result to gout as this requires triggers that build up uric acid in the blood,” Enicola said.
Prior studies show that eating legumes are not associated with gout, even if some legumes have low to moderate levels of purines like stringbean, chickpea, and mungbean; and soy food such as tofu. This is because the purine content of legumes is not as high as those coming from animal-based foods.
“Results of some of the most recent studies and even existing data show that there is no reason why the public, with or without gout, should avoid eating soybeans and soy-based foods when in fact, they provide plentiful amounts of high-quality protein,” Enicola added.
Enicola presented several scientific studies to support the claim that intake of purines from animal sources increases the risk of gout.
In a 2004 study, “Purine-Rich Foods, Dairy and Protein Intake, and the Risk of Gout in Men”, the results reveal that higher levels of meat and seafood consumption are the ones associated with increased risk of gout. Meanwhile, moderate intake of purine-rich vegetables or protein is not associated with increased risk of gout.
Another study in 2005, “Intake of Purine-Rich Foods, Protein, and Dairy Products and Relationship to Serum Levels of Uric Acid”, found that higher levels of meat and seafood consumption are associated with higher serum levels of uric acid.
In a more recent study in 2012, wherein purine-rich foods, protein intake, and the prevalence of hyperuricemia were looked into, it showed that the “intake of soy products (bean curd/tofu, fried bean curd, vegetarian chicken, and bean curd cake and soy milk) was associated with lower risk of hyperuricemia”. Also, it was reported that seafood intake (fish and shellfish combined) was associated with higher prevalence of hyperuricemia.
With these significant findings, Enicola enjoined the public to watch what they eat and modify certain dietary consumptions to include eating “purine-rich” vegetable food from plants like soybean. He also encouraged the public to limit the intake of high purine foods, most of which come from animal source (red meat and liver), and include legumes (including soyfoods) in the daily diet.
BAR, being the focal agency of the Department of Agriculture (DA) for the Soybean R&D Program, is consistent in its promotion of the healthful benefits of soybean and their impact on the soybean industry in the country. Currently, the bureau is supporting the implementation of various soybean projects (production and processing) to further boost the industry and make the public aware of the benefits of eating soybean. (Rita T. dela Cruz, DA-BAR)
- See more at: http://news.pia.gov.ph/index.php?article=1781393825548#sthash.ubJBWSN0.dpuf

Recent Articles
-
Tony
May 08, 24 08:57 PM
Hi Peter, I am a physician, had my first Gout episode last week. I was surfing through the web and happened to come across your site. I am impressed by -
What is it about Cherries?
Aug 25, 21 03:59 AM
Allopurinol worked for me, but at the expense of adversely affecting my mood.I like cherries, but getting them every day of the year is a problem.I wondered -
ACV made my gout worse...
Apr 22, 20 07:19 AM
During my first gout attack, I was in so much pain that I desperately scoured the internet for alternative cures as the colchicine that I was prescribed
